Introduction
Before I start talking about quitting smoking, I want to acknowledge that it isnt easy. Nicotine is very addictive, and everyone smokes for their own reasons. Everyone has a habit they would like to break: mine is enjoying too much chocolate. To stop doing anything which you enjoy takes guts and a lot of will power. Maybe your baby is your reason to quit but it also needs to be because YOU want to not just because you have been TOLD to. I hope this information helps you but always happy to help if you want to email me wendy@breastfeeding-and-medication.co.uk
Smoking in Pregnancy
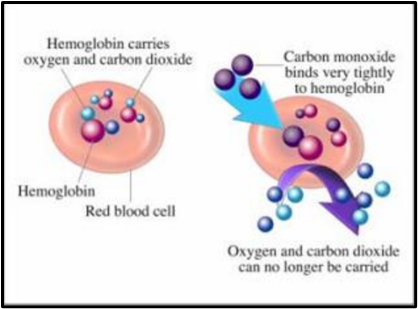
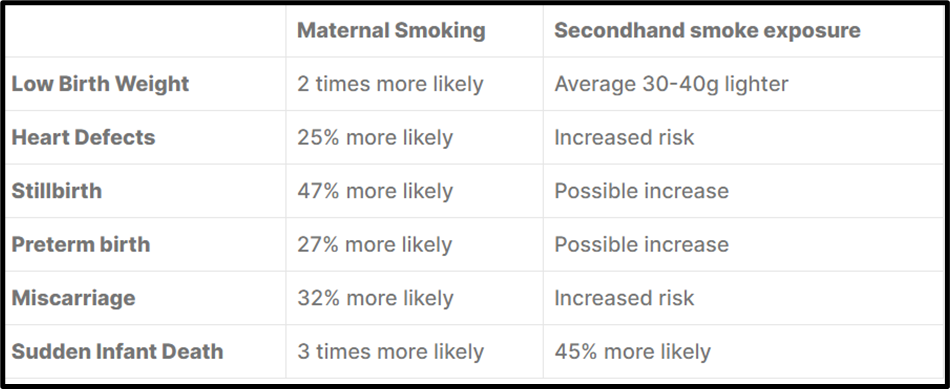
We know that smoking during pregnancy is associated with risk factors to the baby including low birth weight at delivery, increased risk of miscarriage or stillbirth because carbon monoxide in tobacco smoke reduces the amount of oxygen getting to the placenta and the baby . There are also future risks of respiratory problems including ear, nose and throat. However as at 2020/21 9.5% of women were smoking at the time of delivery which was the lowest on record.
In a 2010 study by the Office of National Statistics (ONS) 14% of women were smoking before pregnancy but gave up, 12% continued to smoke throughout pregnancy although 9% cut down. The study showed that 1% gave up but went back to smoking during the pregnancy.
A report published by the Royal College of Physicians in 2010 estimated that in the UK, smoking during pregnancy causes up to 5,000 miscarriages, 300 deaths around the time of birth and approximately 2,200 premature births each year.
(taken from https://ash.org.uk/resources/view/smoking-pregnancy-and-fertility)
Why do mothers smoke during pregnancy?

Why, might we ask, knowing that smoking during pregnancy is harmful to the baby do so few expectant mothers not quit? The answer is very simple: nicotine is extremely addictive and it is hard to break the habit of smoking. Just as overwight people know that they need to lose weight, try to diet but often return to their original weight or more.
Smoking is often linked to deprivation and women may smoke because they cannot afford to eat. If you live with someone else who smokes, you are six times more likely to smoke throughout pregnancy. Additionally, those who live with a smoker and manage to quit are more likely to relapse once the baby is born. If all your friends smoke, especially if you are younger, it is much harder to quit so peer pressure has much to answer to.
How can you stop smoking?
Over half (53%) of the women in a large 2010 study had been given information on how to stop smoking, and a third had received information on how to cut down smoking (32%) and how their partner could stop smoking (33%) but still had not quit. Maybe you have been given the information and now want to quit but have felt “nagged” into doing so when you aren’t ready?
Midwives, pharmacists, GPs as well as smoking cessation clinics can provide nicotine replacement products. These are free on the NHS whilst you are pregnant.
In April 2023 Health Minister Neil O’Brien announced that following the success of local schemes, pregnant women will be offered financial incentives to help them stop smoking. This will involve offering vouchers, alongside behavioural support, to all pregnant women who smoke by the end of 2024.
Nicotine replacement therapy

You can use nicotine replacement therapy (NRT) during pregnancy if it will help you stop smoking and you’re unable to stop without it. It’s not recommended that you take stop smoking tablets such as Champix or Zyban during pregnancy.

Smoking cessation interventions have been shown to reduce the number of new-borns with low birth weight and preterm births. In one study, compared to ongoing heavy smoking, quitting was associated with a 299g increase in birth weight. The less a premature baby weighs at birth the more interventions it is likely to need and the longer it will stay in NICU (neonatal intensive care unit).
NRT contains only nicotine and none of the hundreds of other damaging chemicals found in cigarette smoke. Tobacco smoke contains over 7,000 chemical compounds. NRT is a better option than continuing to smoke. It helps you by giving you the nicotine you would have had from a cigarette whilst you break the habit of reaching for a cigarette ( see below for how to break the habit of smoking).
NRT is available as:
- Patches (The 16-hour NRT patches are preferred to the 24-hour period ones)
- gum
- inhalator
- nasal spray
- mouth spray
- oral strips
- lozenges
- micro tabs
Sometimes a combination of a sustained release patch together with a rapid delivery method works well. As a pharmacist smoking cessation advisor, I often found that the people I was working with found it easier if they had something to hold in their mouths or their hands, so benefitted from an inhalator even if it didn’t contain a product.
Vaping and pregnancy

The vapour from an e-cigarette does contain some of the potentially harmful chemicals found in cigarette smoke, but at much lower levels. If using an e-cigarette helps you to stop smoking, it is much safer for you and your baby than continuing to smoke.
E-cigarettes may be more effective than nicotine patches for pregnant women trying to quit smoking, research found. One major study did not raise any new safety concerns with e-cigarettes (vaping) in pregnancy.
Smoking and breastfeeding
- Nicotine is found in breastmilk of mothers who smoke together with Cotinine, Cadmium, Mercury, Lead and other heavy metals, and a lower amount of proteins, Vitamin A, C and E and other antioxidants.
- The flavour of breastmilk collected 30-60 minutes after smoking was identified as tasting more like cigarettes than samples taken at any other time.
- The levels of cotinine (the chemical into which nicotine is changed in the body) in the urine of breastfed babies whose mothers smoked were ten times higher than those of formula fed babies of smoking mothers. It appears that this is due to passage through breastmilk and not through exposure to smoke in a room.
- Babies of mothers who smoke appear to be more likely to suffer from colic.
- Smoking appears to lower breastmilk production by reducing prolactin levels. More women who smoke believe that they have insufficient milk than non-smokers.
- Mothers who smoke are likely to breastfeed for a shorter length of time.
- Many women continue to smoke whilst breastfeeding perceiving that it is the only time that they have for themselves, to overcome tiredness or to reduce their appetite.
- Passive smoking is related to early onset of wheezing although breastfeeding may reduce the severity of bronchial asthma. Research has shown that babies of mothers who smoke have three times more visits to GP with respiratory and sinus infection and allergy including asthma.
- Research shows exposure to smoke increases the risk of cot death in babies. If the mother and father smoke the risk is multiplied by seven.
- There have been reports linking smoking during breastfeeding with risk of obesity and endocrine dysfunction in the baby in later life.
So, there is no doubt that continuing to smoke whilst breastfeeding is harmful to your baby even if you or your partner don’t smoke in the same room as the baby, maybe even outside. Having said that breastfeeding and smoking still has benefits over not breastfeeding at all.
Behavioural Support
Behavioural support involves regular meetings with a trained person, usually a smoking cessation advisor. You are more likely to quit and remain as a non-smoker with behavioural support rather than trying to quit alone. The therapy is normally offered weekly for 4 weeks. It has also been called motivational interviewing – to help you stay motivated to quit. Normally the level of carbon monoxide (CO) in exhaled breath will be measured to show that you are quitting and as a positive feedback for you as you see the levels fall.
As an advisor I found on several occasions that I had a positive CO level at the end of the session, despite never having smoked, due to inhalation of second-hand smoke of the clients I was supporting many of whom had “one last cigarette” before the appointment!
How to change the habit of picking up a cigarette
We know that nicotine is highly addictive. However, with NRT there may still be a craving to pick up a cigarette at the times that you have normally smoked. These times may be a routine e.g., after a cup of coffee, after a meal. Think about where you smoke – is it always in the same place e.g., a chair you sit in, outside the kitchen door so in sight or sound of your baby but not with him/her.

It can help to identify when these times are for you and where you tend to smoke. I recommend keeping a diary for a week during which time you can also think about why you have decided to quit – is it for your baby, for your own health, because of the cost? Is it because you think you OUGHT to or have been told you SHOULD do so. If this has happened how do you feel about that? Shoulds and oughts are often hard to maintain. Plan to stop smoking rather than making a rapid decision on the spur of the moment, even with the best of intentions.
Decide how you can change each time you smoke – can you distract yourself for 20 minutes? This is the time it usually takes a craving to subside. Could you wash the floor, sing a song to your baby, make everything ready for the next meal, paint your nails or something else that works for you? If you smoke to give yourself “5 minutes peace” think about how else you could spend that time positively for you even if it is only to wee by yourself!
On the day you decide to stop, you may choose to tell everyone so that you gain their support, or you may want to keep quiet, so no-one tries to tempt you because they haven’t made their own decision. Some people just want to prove how hard it is and set you up to fail. Only you know whether your friends and family will help you or not.
I would also suggest putting the money that you would have spent on cigarettes in a savings box and at the end of 4 weeks or whatever period you decide, treat yourself to something you would have otherwise not been able to afford. Of course, you might choose that to be a family treat but remember it is also rewarding you for beating the addiction and craving. It isnt easy to give up smoking so be proud of yourself.
IF you have a cigarette one day at a point of weakness, be kind to yourself, accept the slip but carry on your intention to stop – one cigarette doesn’t mean you have failed, it is just one cigarette. Don’t stop giving up!
Have strong tasting sweets around to suck – traditionally these are mints but could be anything you like. Also have lots of healthy snacks so you don’t resort to chocolate or high calorie foods instead.
Nicotine Replacement Therapy (NRT) and Breastfeeding

- It is safer to use nicotine replacement therapy whilst breastfeeding than to smoke.
- Babies will be exposed to less nicotine through NRT than through smoking. Smoking produces blood levels of nicotine of 44ng/ml whilst NRT patches produce around 17 ng/ml.
- NRT avoids exposure to the other chemical compounds in tobacco smoke.
- Patches applied over a 24-hour period may produce vivid dreams in the mother; it might be advisable to remove the patch overnight so that the baby is exposed to less during night time feeds.
- NRT products do not cause breastmilk to smell of cigarettes.
- Nicotine gum produces large variations in nicotine levels whilst patches produce a sustained but lower level. If gum is used it should be chewed immediately after feeds to reduce the baby’s exposure. NRT nasal sprays similarly produce rapid high levels and may best be used after feeds.
- Exposure of the baby to NRT products is safer than exposure to cigarettes and with appropriate support may help the mother (and ideally her partner) to quit smoking permanently.
Medications to stop smoking and breastfeeding.
These tablets are not generally advised during breastfeeding but everyone has individual needs and they might be what is right for you.
Champix™ ( Varenicline)
• Varenicline is a partial nicotine agonist used to assist smoking cessation.
• One researcher points out that based on animal data on nicotine, varenicline might interfere with normal infant lung development and recommends against its use in nursing mothers.
• Based on its long half-life, poor protein binding and small molecular weight it is anticipated to transfer to human milk.
• Because no information is available on the use of varenicline during breastfeeding, an alternate drug is preferred, especially while nursing a new-born or preterm infant.
• If used monitor the baby for changes in sleep, changes in feeding, vomiting, constipation.
• For more information https://www.ncbi.nlm.nih.gov/books/NBK501688/
Zyban ™ (Bupropion)
• Limited information indicates that maternal bupropion doses of up to 300 mg daily produce low levels in breastmilk and would not be expected to cause any adverse effects in breastfed infants.
• However, there is little reported use in breastfed new-born infants and case reports of a possible seizure in partially breastfed 6-month-olds.
• If bupropion is required by a nursing mother, it is not a reason to discontinue breastfeeding.
• However, another drug may be preferred, especially while nursing a new-born or preterm infant.
• For more information https://www.ncbi.nlm.nih.gov/books/NBK501184/
Vaping and breastfeeding
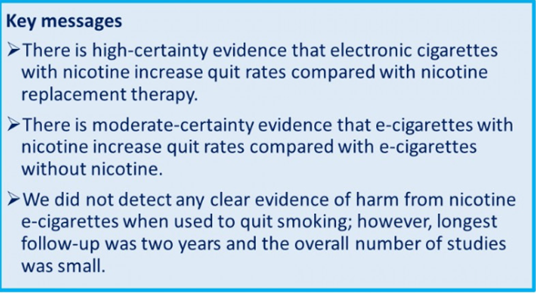
A Cochrane review has found the strongest evidence yet that e-cigarettes, also known as ‘vapes’, help people to quit smoking better than traditional nicotine replacement therapies, such as patches and chewing gums.
E-cigarettes have become very popular as a safer alternative to cigarette smoking without exposure to tobacco and substances known to cause detrimental effects including lung cancer.
It was reported that an e-cigarette produced peak blood nicotine levels of 1.3 ng/mL in 19.6 minutes, which is comparable to the levels obtained by a nicotine inhaler (2.1 ng/mL in 32 minutes) and much lower than those obtained by a conventional cigarette (13.4 ng/mL in 14.3 minutes). This study further revealed that the reduction in the desire to smoke is similar to that of a nicotine inhaler but that e cigarettes are better tolerated by users.
The amount of nicotine delivered after 10 puffs of a 16 mg e cigarette is little to none. Based on these findings, it can be concluded that the amount of nicotine that transfers into breast milk after an acute inhalation of an e-cigarette is probably minimal, and comparable to that of a nicotine inhaler. But it is reported that an average e-cigarette user inhales up to 120 puffs/day.
Celebrate
Be proud of yourself – stopping smoking is not easy! Take every day as it comes and celebrate.

References
- Bullen C, McRobbie H, Thornley S, Glover M, Lin R, Laugesen M. Effect of an electronic nicotine delivery device (e cigarette) on desire to smoke and withdrawal, user preferences and nicotine delivery: randomised cross-over trial. Tob Control. 2010 Apr;19(2):98-103.
- Eissenberg T. Electronic nicotine delivery devices: ineffective nicotine delivery and craving suppression after acute administration. Tob Control. 2010 Feb;19(1):87-88)
- Etter JF, Bullen C. Electronic cigarette: users’ profile, utilization,satisfaction and perceived efficacy. Addiction. 2011 Nov;106(11):2017-2028
- Gov.UK Smokers urged to swap cigarettes for vapes in world first scheme https://www.gov.uk/government/news/smokers-urged-to-swap-cigarettes-for-vapes-in-world-first-scheme
- NHS Digital Statistics on Women’s Smoking Status at Time of Delivery: England Quarter 4, 2020-21
- NHS Stop smoking in pregnancy https://www.nhs.uk/pregnancy/keeping-well/stop-smoking
- NIHR Smoking and Addiction https://evidence.nihr.ac.uk/alert/e-cigarettes-better-than-nicotine-patches-helping-pregnant-women-stop-smoking/
- Tappin D, Sinclair L, Kee F, McFadden M, Robinson-Smith L, Mitchell A et al. Effect of financial voucher incentives provided with UK stop smoking services on the cessation of smoking in pregnant women (CPIT III): pragmatic, multicentre, single blinded, phase 3, randomised controlled trial BMJ 2022; 379 :e071522 doi:10.1136/bmj-2022-071522
- Zhao L et al. Parental smoking and the risk of congenital heart defects in offspring: An updated meta-analysis of observational studies. 2020; RCP. Hiding in plain sight: treating tobacco dependency in the NHS. 2018; Pineless BL et al. Systematic review and meta-analysis of miscarriage and maternal exposure to tobacco smoke during pregnancy. 2014; RCP & RCPCH. Passive Smoking and Children. 2010