Sadly our family has experienced the tragedy of an ectopic pregnancy and the loss of a very brief dream. This has made me much more aware of the incidence and risk of this condition over. So some more facts – as my friend commented today I hate to waste any opportunity to educate!
I have also heard from several mothers who have been diagnosed with an ectopic pregnancy. They have variously been told that they cant breastfeed again for 2 months and 3 months. One distraught mother planned to pump and dump her milk for 3 months with the hope that she could return to breastfeeding later.
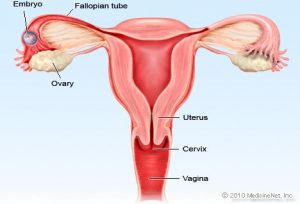
Ectopic pregnancy is a common, occasionally life-threatening condition, that affects 1 in 80 pregnancies. An ectopic pregnancy is when a fertilised egg implants itself outside of the womb, usually in one of the fallopian tubes. Symptoms usually develop between the 4th and 12th weeks of pregnancy. Women with an ectopic pregnancy may still be breastfeeding and wish to continue which can be supported.
Symptoms
- Ongoing bleeding that is sometimes red or brown/black and watery (like “prune juice”) should be investigated. The bleeding may be heavier or lighter than usual, but pregnancy test is still positive
- One-sided pain in your tummy which may be persistent or intermittent or a generalised discomfort with bloating and a feeling of fullness (not associated with eating) when lying down.
- Shoulder tip pain which is often described as pain unlike any you have ever experienced before. (Ectopic Pregnancy Trust)
Investigations
Your GP will refer you urgently to the early pregnancy unit at your local hospital. You may have your Human Chorionic Gonadotropin (HCG levels) measured over a period of several days. If you are having a normal pregnancy these should double approximately every 48 hours. A smaller increase can indicate a risk of of this being an ectopic pregnancy but this will be confirmed with ultrasound scans, initially across your tummy. It is likely that a transvaginal (internal) ultrasound scan will be required where a specialised probe is placed into the vagina to get a more detailed look at the reproductive organs.
Unfortunately, if it is confirmed over a period that you have an ectopic pregnancy it is not possible to save the pregnancy and it must be removed either by surgery or the use of methotrexate. The cells have not been able to be nourished and can never develop into the baby you thought you were expecting which can be hard to deal with.
Rupture of ectopic pregnancy
In a few cases, an ectopic pregnancy can grow large enough to split open the fallopian tube. This is known as a rupture which can be very serious, and surgery needs to be carried out as soon as possible.
Signs of a rupture include a combination of:
- a sharp, sudden and intense pain in your tummy
- feeling very dizzy or fainting
- feeling sick
- looking very pale (NHS Choices)
Methotrexate and breastfeeding
Mothers who are currently breastfeeding an older child can continue 24 hours after the methotrexate is administered.
“It is apparent that the concentration of methotrexate in human milk is minimal, although due to the toxicity of this agent and the unknown effects on rapidly developing neonatal gastrointestinal cells, it is probably wise to pump and discard the mother’s milk for a minimum of 24 hours post dose if given as a single dose (e.g. 50 mg/m2 IM for ectopic pregnancy).
The period in which the mother discards her milk may require extending (consider 4 days of interruption) if the dose used is quite high (>75mg). (Hale 2023). This is due to lack of data from research on accumulation in infant tissues rather than levels in breastmilk.
In a case report of a woman receiving 92 mg IM daily for 3 days (Baker T, Datta P, Rewers-Felkins K, Hale TW. High-dose methotrexate treatment in a breastfeeding mother with placenta accreta: a case report. Breastfeed Med. 2018 Jul/Aug;13(6):450-452 ), milk levels were collected and assayed for methotrexate although she was advised not to breastfeed.dose. Both methotrexate and its metabolite 7-hydroxymethotrexate levels in milk were exceedingly low. On day 2 of therapy, the average milk concentration of methotrexate was 8.6 ng/mL. The maximum concentration of methotrexate occurred at 2 hours and was found to be 16.9 ng/mL. The levels gradually receded and were 4.9 ng/mL at 24 hours. The relative infant dose of methotrexate (RID) was calculated at 0.11%. The half life of methotrexate is quoted as 8-15 hours (Hale 2023).
Infant Monitoring: Should patient resume breastfeeding more than 24 hours after the last dose of maternal therapy, monitor the infant for vomiting, diarrhoea, blood in the vomit, stool or urine. Lab work could be drawn if clinical signs of liver or renal dysfunction, anaemia, thrombocytopenia or an inability to fight infection.
Lactmed reports a study of one mother who was given a single intramuscular dose of 65 mg (50 mg/square meter) of methotrexate for ectopic pregnancy. Six milk samples were obtained from 1 to 24 hours after the dose. Methotrexate was undetectable (<22.7 mcg/L) in all milk samples (Tanaka 2009). In some 20% of cases more than one cycle of methotrexate is required to expel the products of conception. For each cycle breastfeeding should be avoided for 24 hours.
Hale quotes a milk plasma ratio of > 0.08 and relative infant dose of 0.13% – 0.95%. Peak serum concentrations appear 30-60 minutes after intra muscular dose (Jones 2018). Pharmacokinetic data is very variable as there in considerable inter individual variation (Martindale 2017).
Methotrexate and breastfeeding
There is not much information about methotrexate and breastfeeding, but it shows that methotrexate passes into breast milk in tiny amounts. Your doctor or specialist will advise what’s best for you and your baby.
If your weekly dose of methotrexate is 25mg or less, it may be possible to breastfeed. However, you must not breastfeed for 24 hours after taking your medicine. Your midwife or health visitor can give you advice about how to feed your baby while you wait 24 hours. https://www.nhs.uk/medicines/methotrexate/pregnancy-breastfeeding-and-fertility-while-taking-methotrexate/
Ectopic pregnancy and breastfeeding fact sheet
Breastfeeding after surgery
After surgery breastfeeding can continue as normal as soon as you are awake and alert. If your nursling is unable to stay in hospital with you, you may need to express to avoid engorgement/blocked duct and to maintain your supply. Your expressed milk can be given to your baby at home. There is no need to pump and dump.