I am so very frustrated for breastfeeding mothers who need colonoscopies and endoscopies being told that they need to interrupt breastfeeding. I was able to engage with the national body to update national guidelines which should be released soon.
Interestingly it is the same old story – we dont see breastfeeding women needing these examinations. So how come I do?
Some 3 years ago I began working with British Society of Gastroenterology on guidelines for sedation in gastrointestinal endoscopy. Much of the review was outside of my experience but I remain an author of the paper “British Society of Gastroenterology guidelines on sedation in gastrointestinal endoscopy. It was published in BMJ Gut in October 2023. As regards sedation in breastfeeding mothers it recommends:
47. We recommend that breast feeding does not need to be suspended after a single intravenous dose of midazolam, fentanyl or pethidine or when used in combination, or after administration of propofol.
Grade of evidence: Low. Strength of recommendation: Strong.
Level of agreement: 100%
This guideline superceedes the information from 2012 (Shergill et al ASGE)
What are lactating mothers currently advised following procedures?
Many mothers who are lactating are questioning information provided by their gastroenterology team about lactation (18 queries identified in 6 weeks July and August 2020 to the Breastfeeding Network Drugs in Breastmilk service). In each case the mothers had been advised in three different ways:
- To stop breastfeeding during bowel preparation
- That they should stop breastfeeding for 24 hours after sedation for either procedure
- Or that if they were unwilling to stop breastfeeding after sedation that the procedure could only be undertaken with gas and air as analgesia
Whilst it is accepted that not all patients need sedation in order to undertake colonoscopy or endoscopy these women were not offered the choice.
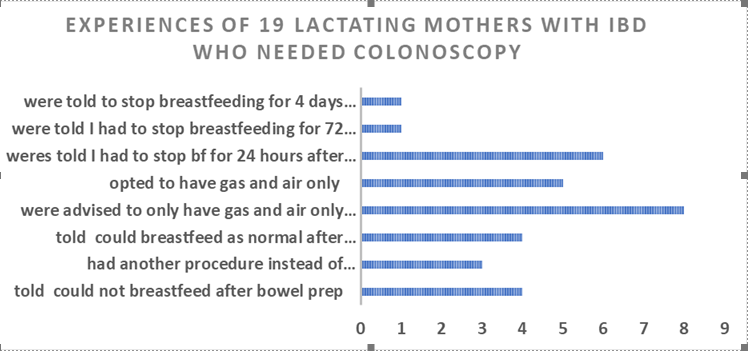
This data has not changed significantly from a study published as a poster at the Baby Friendly Initiative Conference 2016
In that data 19 emails to the Drugs in Breastmilk helpline over a 6-month period February – August 2016 were analysed. All 19 mothers were already diagnosed with Inflammatory Bowel Disease (Ulcerative Colitis or Crohns Disease). Details of the duration advised to interrupt breastfeeding were noted together with comments made by the mothers about their care.
Quotes From Mothers
- My daughter will not take anything from a bottle or cup at the moment
- I am very worried that if I do not feed him for 2 days that my already tenuous supply will dwindle. (Baby 20 weeks)
- Their imaging department have been quite adamant that I cannot breastfeed for at least 24 hours but cannot explain to me why
- I also co-sleep with my baby at night and am concerned to only do this safely, this is currently the only way my baby will sleep at night.
- I am not sure I want to express that much as I do not want to mess with my supply
- The consultant I see is not very sympathetic to me wanting to continue breastfeeding and just told me I need to choose between feeding my baby or being well.
- I will proceed without any pain relief but wondered if there might be an alternative?
- I am worried I should try and cancel the procedure
- It has been suggested maybe I delay it until not breastfeeding, but I want to continue
- I had a colonoscopy today after switching hospital. It was wonderful to be treated with care and respect. I feel so much happier. I would recommend asking your GP for a referral for a different hospital if you are not happy with your care.
- It took us 8 weeks to latch and now at 15 weeks I am not going to go back to pumping all day when it is not essential.
- I know I can breast feed but not keen to starve myself for 24 hours and dehydrate myself. She then said as my little girl has turned one it is probably me feeding her that is caused this.
- Starting to doubt myself as some family members not happy
Summary Of Mother’s Comments
There are recurrent themes of:
- feeling that their breastfeeding is dismissed as unimportant by the specialist team
- concerns about supply or impact on risk of engorgement/mastitis
- Worries about how they will cope on liquid diet only when breastfeeding and caring for a baby
- That the mothers will endure pain and discomfort by coping without pain relief or just with gas and air rather than interrupt breastfeeding
- Concern from other family members about risk to the baby
There is no research to support the belittling of the importance in a breastfeeding an older baby and may represent a need to improve the education of medical professionals to the importance of breastmilk to protect mother and baby (Walters 2019). Indeed, WHO guidance supports the use of breastmilk as part of the diet of a child to 2 years and beyond. There is a link between formula feeding and IBD (Whorwell 1979, Xu 2017)
Midazolam
Matheson (1990) studied 12 women prescribed midazolam orally for sleep in the first 5 days after delivery. In 11 of the mothers the midazolam was undetectable in breastmilk 7 hours after the dose ((<3 mcg/L). However, in the first 5 days after delivery the gaps between cells are wide open to allow passage of immunoglobulins to pass through into milk with ease. This inevitably means that all other medication administered at this time will similarly pass readily into milk. That levels were below the level of detection after 7 hours at this stage supports the hypothesis that the drug does not readily transfer to the baby.
Nitsum (2006) studied 5 women 6-15 weeks post-partum given 2 mg pre- operatively (IV). The researchers estimated that the infants would receive an average of 0.016 mcg/kg in the 24 hours after a single dose of midazolam (0.06% of the maternal weight-adjusted dosage) and that this would be unlikely to affect a healthy, term baby.
Lee (1993), Spigsett (1994) and Nitsum (2006) recommend that after a single dose of midazolam that the mother may resume breastfeeding as soon as she is awake and alert following anaesthesia (LactMed).
Midazolam is extensively plasma-protein bound (97%) and poorly bioavailable (40-50%). (Brown 2019). Half life 3 hours so all removed from the body in 15 hours (5 half-lives).
Fentanyl
In Nitsum (2006) study the 5 the median amount of fentanyl recovered in milk within 24 hours post dose was 0.024 µg or 0.024% of the maternal dose women undergoing surgery and he recommended that mothers could breastfeed as normal thereafter. Oral bio availability 50-75% (Brown 2019).
Meperidine/Pethidine
Meperidine/ Pethidine has historically widely been used in labour. In a neonate the metabolite normeperidine it has a prolonged half-life (63 hours) but after 6 weeks returns to that of the adult (15-30 hours). Borgatta (1997) studied 9 women undergoing surgery for tubal ligation and concluded that a single dose for anaesthesia or conscious sedation usually does not cause problems in older breastfed infants. Meperidine/pethidine is only 50% orally bio-available (Brown 2019).
Propofol
Mitchell et al (2020) minimal amounts (0.025%) of propofol are transferred to breast milk. This is not a concern even when propofol is used by infusion for maintenance of anaesthesia. Breastfeeding may be resumed as soon as the woman has recovered sufficiently from general anaesthesia (Allegaert 2015).
Bowel preparations
Macrogols: the most commonly used laxative agents to clear the gut are Movicol ™and Laxido ™ otherwise known as polyethylene glycol- electrolyte solution. They are saline laxative which are not absorbed from the gut but pull water into the bowel to wash the contents out. Because it is not absorbed from the gut it cannot get into breastmilk and would not affect the baby. They are licensed to be used during breastfeeding
Sodium picosulfate (Picolax ™): is not absorbed from the gastrointestinal tract, and its active metabolite, which is absorbed, is not detectable in breastmilk. Breastfeeding can continue as normal.
Macrogol 3350 (KleanPrep ™): contains, an osmotic laxative with a high molecular weight and zero oral bioavailability. Like Moviprep it accumulates water into the GI tract, where it acts as a laxative. It would be very unlikely to enter the plasma of the mother, or milk. Senna: is a stimulant laxative. Its key ingredient (anthraquinone), is believed to increase bowel activity due to secretion into the colon. It may produce abdominal cramps. In one study of 23 women who received Senokot none was detectable in their milk.[1] Of 15 mothers reporting loose
stools, two infants had loose stools (Werthmann 1973). However, in a randomized, double-blind trial comparing Senokot tablets to placebo, of the women in the study, 126 breastfed their infants and took senna while 155 control mothers breastfed their infants. There was no difference in the percentages of infants in the active and control groups with loose stools or diarrhoea (Shelton 1980). In this study 8 doses were taken. In bowel preparation a single dose only is used.
Sodium phosphate enema (Fleet™): is a saline laxative which sucks water into the lumen of the bowel. Whilst some phosphate may get into the plasma, it is very unlikely to change the levels in milk. The oral bioavailability is zero to 20%. Use of phosphate enemas should not require interruption of breastfeeding (LactMed)
Bisacodyl (Dulcolax ®): is poorly absorbed from the gut (oral bioavailability <5%) and so reaches low levels in breastmilk. It is a stimulant laxative. Breastfeeding can continue as normal
Conclusion
There is no evidence to support the recommendation to delay breastfeeding after endoscopy or colonoscopy or after bowel cleansing for colonoscopy in a healthy, term infant.
References
- Allegaert K, van den Anker JN. Maternal analgosedation and breastfeeding: guidance for the pediatrician. Journal of Pediatric and Neonatal Individualized Medicine 2015; 4: e040117.
- Borgatta L, Jenny RW, Gruss L, et al. Clinical significance of methohexital, meperidine, and diazepam in breast milk. J Clin Pharmacol. 1997; 37:186–92.
- LactMed National Library of Medicine, Drugs and Lactation Database
- Lee JJ, Rubin AP. Breast feeding and anaesthesia. Anaesthesia. 1993; 48:616–25.
- Matheson I, Lunde PKM, Bredesen JE. Midazolam and nitrazepam in the maternity ward: milk concentrations and clinical effects. Br J Clin Pharmacol. 1990; 30:787–93.
- Mitchell J, Jones W, Winkley E, Kinsella. S.M Guideline on anaesthesia and sedation in breastfeeding women 2020. Guideline from the Association of Anaesthetists. First published: 01 August 2020 https://doi.org/10.1111/anae.15179
- Nitsun M, Szokol JW, Saleh HJ, et al. Pharmacokinetics of midazolam, propofol, and fentanyl transfer to human breast milk. Clin Pharmacol Ther. 2006; 79:549–57. [PubMed]
- Shelton MG. Standardized senna in the management of constipation in the puerperium. A clinical trial. S Afr Med J. 1980; 57:78-80. Brown A and Jones W A guide to supporting breastfeeding for the medical profession Routledge (2019)
- Shergill AK, Ben-Menachem T, Chandrasekhara V, et al. Guidelines for endoscopy in pregnant and lactating women GASTROINTESTINAL ENDOSCOPY 2012;76 (1): 18-24)
- Sidhu R, Turnbull D, Haboubi H, et al British Society of Gastroenterology guidelines on sedation in gastrointestinal endoscopy Gut Published Online First: 10 October 2023. doi: 10.1136/gutjnl-2023-330396
- SPC Hypnovel https://www.medicines.org.uk/emc/product/10948/smpc
- Spigset O. Anaesthetic agents and excretion in breast milk. Acta Anaesthesiol Scand. 1994; 38:94–103.
- Walters, D, Phan, LTH, & Mathisen, R, (2019). The cost of not breastfeeding global results from a new tool, Health Policy and Planning, doi.org/10.1093/heapol/czz050
- Werthmann MW Jr, Krees SV. Quantitative excretion of Senokot in human breast milk. Med Ann Dist Columbia. 1973; 42:4-5.
