PDF of this information is available at:
See also The Management of Nausea and Vomiting in Pregnancy and Hyperemesis Gravidarum (Green‐top Guideline No. 69) – Nelson‐Piercy – 2024 – BJOG: An International Journal of Obstetrics & Gynaecology – Wiley Online Library
The Management of Nausea and Vomiting in Pregnancy and Hyperemesis Gravidarum (Green-top Guideline No. 69) Feb 2024
Thank you to everyone on the facebook group who shared their experiences and helped me to update this information.
More women are now breastfeeding their babies for longer and may still be feeding when they fall pregnant. For those who suffer from hyperemesis gravidarum (HG) this is a tough time. Sadly, some healthcare professionals do not understand that there is benefit to a child from being breastfed to the age of two years and beyond (WHO) alongside a normal weaning diet. Being asked to abruptly wean your older child in order to take medication is not an easy option and is not necessary. Sometimes sitting quietly to breastfeed whilst you fight the feeling of nausea is helpful. Some professionals remain concerned about the teratogenicity of drugs in pregnancy despite national guidance.
“ I had an absolutely awful time while still trying to breastfeed a toddler. The GP refused to prescribe anything other than cyclizine despite me calling them in desperation many times. Nothing else was made available and I was told that I just had to wait until it cleared up.”
Symptoms of NVP and HG
Nausea and vomiting of pregnancy (NVP) is common and usually settles by 12-14 weeks of pregnancy (although it may be longer and even last the full pregnancy). Often known as morning sickness it can occur at any time of the day or last all day.
Hyperemesis gravidarum is a severe form and can affect up to 1 to 3 in 100 pregnant women. Sadly, some women experience such extreme symptoms that they feel that they have no choice but to terminate the pregnancy even if it is a much longed for baby.
“I ended in termination of pregnancy after first hospital visit as I didn’t want to take from my child who was already here and after how badly I dealt with it last time, it being worse instantly I couldn’t do it”
Others decide that one child is sufficient to complete their family as they cannot contemplate symptoms again. There are medications but often primary care professionals do not appreciate the severity of symptoms or impact on mothers.
“I had HG with my daughter who will be 11 next month. Hyperemesis is the primary reason I only have one child. It was physically horrendous, and I had post-traumatic stress for years afterwards”.
“I had this with my daughter. It is the reason she will be an only child. She’s 4 now and I still suffer a lot of health issues as a direct result of hyperemesis. I had the best medical care. And was lucky to be given a lot of treatment. But it wasn’t enough, and my body still struggled. You can’t appreciate how difficult it is until you’ve experienced it.”
When asked in a facebook group (https://www.facebook.com/breastfeedingandmedication) for their experiences of suffering from morning sickness and hyperemesis, one of the overwhelming comments from women was about reluctance of GPs to prescribe medication in pregnancy, even when it had been prescribed whilst the mother was hospitalised!
“After one of my hospitalisations I was sent home with a prescription for cyclizine and when I went to my GP to renew the prescription she talked me out of it because “it wasn’t making enough of a difference for me to go back to work” so didn’t seem worth taking (mild relief from the symptoms of HG wasn’t considered a benefit.)”
Repeated comments from family, friends and professionals underestimated how the woman was feeling and she didn’t feel listened to.
“I didn’t feel I wasn’t listened to and also I didn’t feel dismissed. I just accepted this was part and parcel of my pregnancy as it was just relayed to me that it was normal.”
“It was awful. People (friends, family, healthcare workers) were quick to tell me what worked for them, and I felt very blamed that I was somehow not trying hard enough. All the admissions were almost a relief, just to lie there with fluid going in. I used to be admitted for several days each week, particularly in third trimester. I still have consequences from the prolonged malnutrition.”
For what should be a joyous family time there were repeated descriptions of an awful experience:
“ horrendous, hell on earth, pure hell, absolutely hell, housebound for months, nothing worked”.
“ I wasn’t taken seriously until my organs started to shut down and I needed to be induced, I spent 5 months in bed, couldn’t drink water or anything else, everything made me feel nauseous.”
“ I vomited so much and so hard that every time I wet myself and my nose bled. I was told when I was 5 weeks pregnant that if I didn’t want to be sick I shouldn’t be pregnant. I ended up hospitalized at 8 weeks.”
Should this be the experience of women in the UK in 2023?
Anti emetics in breastfeeding and pregnancy
Many of the drugs used to relieve nausea in pregnancy may be associated with lowering of milk supply. However, most women find that their supply very rapidly diminishes when they are pregnant. Many also develop aversion and very sensitive nipples and wish to limit feeding. Sadly, toddler nurslings don’t always understand the loss of their comfort! Many breastfeeding dyads continue to dry nurse throughout pregnancy and may go on to tandem feed. It is the decision which works for each family which matters, without judgement from family and professionals.
Hyperemesis may result in dehydration and subsequent admission to hospital. Signs of dehydration include feeling very thirsty, becoming drowsy or unwell, urine changing from a light yellow to a dark yellow or brown colour. Medical help should be sought if even sips of fluid produce vomiting. Weight loss can be excessive because of the restriction of quantity of food tolerated. Hyperemesis is diagnosed when there is prolonged nausea and vomiting with more than 5% pre pregnancy weight loss, dehydration and electrolyte imbalance. https://cks.nice.org.uk/topics/nausea-vomiting-in-pregnancy/background-information/definition/
Self-care
https://cks.nice.org.uk/topics/nausea-vomiting-in-pregnancy/management/management/
- Rest as needed and try to avoid sensory stimuli that may trigger symptoms, such as odours, heat, and noise.
- Try eating plain biscuits or crackers in the morning.
- Try eating bland, small, frequent protein-rich meals which are low in carbohydrate and fat.
- Cold meals may be more easily tolerated if nausea is smell-related.
- Drinking little and often, rather than large amounts.
- Ginger (can be taken in fresh, tea, capsule, or syrup form).
- Acupressure (such as over the P6 point on the ventral aspect of the wrist using a wrist band or finger pressure).
Responses on the facebook group as to how helpful these suggestions were are exemplified by:
“Nausea and sickness with my first born I had such a heightened sense of smell. I couldn’t even open my fridge without feeling sick and running to the loo. I ended up using a cool bag instead of my fridge, and I had to call my mum to come and help me when my partner was away. I couldn’t brush my teeth without gagging and wanting to be sick.”
“I was asked what is had to eat and when I said an oat/raisin bar the doctor replied I shouldn’t be having anything sugary. That one doctor who knew her stuff had told me to eat anything I could keep down.”
Medical Treatment
The RCOG green top guidelines on treating are available https://www.rcog.org.uk/media/y3fen1x1/gtg69-hyperemesis.pdf
See also Hyperemesis gravidarum Nana, Melanie et al.The Lancet, Volume 407, Issue 10523, 78 – 89 https://www.thelancet.com/journals/landia/article/PIIS0140-6736(25)01454-0/abstract
Hyperemesis gravidarum describes nausea and vomiting in pregnancy severe enough to cause weight loss, dehydration, electrolyte imbalance, and nutritional deficiencies. The condition can render women so physically and mentally unwell that they are at increased risk of terminating a wanted pregnancy and experiencing suicidal ideation. Concerns regarding prescribing in pregnancy and inaccurate assumptions that the condition is self-limiting result in women being dismissed and having difficulty accessing appropriate care. Over the past decade, a wealth of literature has been published that gives new insights into the causes of hyperemesis gravidarum, the safety of antiemetic therapy, and short-term and long-term consequences for women with the condition and their children. This Review summarises the findings of this literature with the aim of informing decisions about the care of these women and future research priorities.
The UKTIS information on the use of drugs in pregnancy can be found at https://www.medicinesinpregnancy.org/leaflets-a-z/nausea–vomiting/
RCOG Recommended antiemetic therapies and dosages
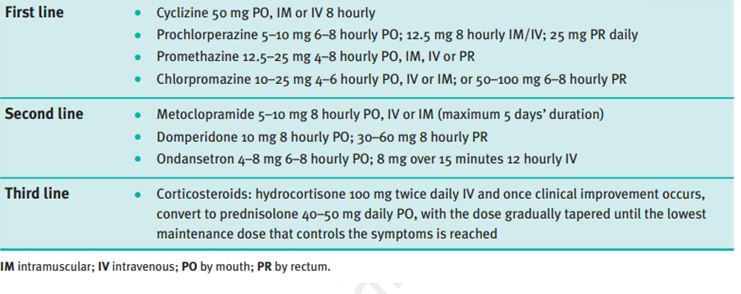
In this fact sheet I have provided links to detailed information on the medication which can help prescribers to reach an evidence-based decision on the safety of the drug to the breastfeeding baby which is not available in standard reference texts like the British National Formulary (BNF). The linked pdf files contain information sourced from LACTMED February 2023
First Line treatments
- Cyclizine (Valoid™)
May possibly cause some drowsiness in the nursling but anecdotally appears to happen rarely . See https://www.ncbi.nlm.nih.gov/books/NBK501749/ and https://www.e-lactancia.org/breastfeeding/cyclizine/product/
Cyclizine is an anti-emetic used to treat nausea and vomiting including motion sickness, post-operative nausea and vomiting, after radiotherapy, in drug-induced situations, as well as for nausea in pregnancy. There are no reports of levels entering breastmilk (BNF) or data on which to base conclusions. There is an unlicenced dose for children aged over 6 years. It may be given orally, by IV or IM every 8 hours. Manufacturers advise to avoid in pregnancy, but there is no evidence of teratogenicity
·
Prochlorperazine (Buccastem, Stemetil)
Low levels of prochlorperazine are secreted into breastmilk and it can be used when breastfeeding. Side effects for the mother include drowsiness, restlessness and occasional extra pyramidal effects but babies seem to exhibit no adverse reactions. It is licensed to be given directly to babies weighing more than 10 kg. See https://www.ncbi.nlm.nih.gov/books/NBK501080/ and https://www.e-lactancia.org/breastfeeding/prochlorperazine/product/
Prochlorperazine is used to treat vertigo, labyrinthitis, migraine or drug-induced emesis if severe vomiting is a problem. Its oral bio-availability is low due to high first-pass metabolism but, like all phenothiazines, it has many metabolites, some active. It is not generally used in travel sickness prophylaxis. It is a member of the phenothiazine family to which children are particularly sensitive. Long-term use should be avoided in breastfeeding where possible, particularly with very young babies where there is a potential risk of apnoea. However, short-term acute use probably poses few risks as it is licenced for use in children over 10 kg. The dose is 5-10mg (one or two tablets) every 6-8 hours. It may also be given IV or IM.
- Promethazine (Avomine™ Phenergan™, Sominex™)
When used for hyperemesis in mother promethazine may possibly cause some drowsiness in the nursling but anecdotally appears to happen rarely. It also causes drowsiness in the mother so care should be taken with co sleeping.
See https://www.ncbi.nlm.nih.gov/books/NBK501081/ and https://www.e-lactancia.org/breastfeeding/promethazine/product/
Promethazine is widely used to reduce nausea particularly associated with travel sickness as well as symptomatic relief of urticaria and as an over-the-counter (OTC) hypnotic for short-term use. No data are available on transfer into breastmilk but it is believed that it does pass into breastmilk. It is licenced for use in children over 2 years.”
· Doxylamine/pyridoxine (Xonvea™, Cariban™)
This is the only licensed drug treatment for nausea and vomiting of pregnancy. It contains a combination of the antihistamine doxylamine and the vitamin pyridoxine. It became available in England in 2018. It has been widely used for pregnancy sickness in the US and Canada and studies have shown no link with birth defects in the baby. The antihistamine doxylamine might be more likely to cause drowsiness in nursling. https://www.ncbi.nlm.nih.gov/books/NBK500620/ and https://www.e-lactancia.org/breastfeeding/doxylamine-succinate/product/. The 10mg of pyridoxine is unlikely to cause any disruption to breastfeed.
Second Line Treatments
· Metoclopramide (Maxolon™)
Metoclopramide has also been used to increase milk supply. It is associated with an increased risk of depression as well as other side effects if used long term. There are no reports of problems in the babies from the amount passing through breastmilk. https://www.ncbi.nlm.nih.gov/books/NBK501352/
Metoclopramide is a dopamine antagonist and can cause extra-pyramidal side effects, in particular acute dystonia. This adverse effect is most commonly seen in children and young adults, especially females, so it is not a drug of choice in lactating mothers who generally fall into this age group. It may also precipitate hypotension and depression. Other side effects reported include headache, diarrhoea, dry mouth and change in appetite (Ingram et al. 2011). It stimulates prolactin secretion and has been used as a galactogogue but has now been superseded by domperidone because of the latter does not cross the blood–brain barrier (Ingram et al. 2012). The bio-availability of oral metoclopramide is about 75% but varies widely between patients due to its hepatic first-pass metabolism. Concentrations higher than those in maternal plasma may be reached in breastmilk, particularly in the early puerperium, although these decrease with increased maturity. Metoclopramide has pro-kinetic and anti-emetic properties and acts directly on the gastrointestinal tract without altering acid secretion. It is more frequently used in the US where domperidone is not available. Relative infant dose is quoted as 4.7–14.3% (Hale online access). The BNF states that only a small amount is present in breastmilk but it should be avoided.
· Domperidone (Motilium™)
Domperidone has widely been used to increase milk supply in the past. Concerns were raised by the MHRA in 2014 about use in patients with heart defects, there has been some reticence by doctors to prescribe it. There are no reports of problems in the amounts passing through breastmilk
See https://www.ncbi.nlm.nih.gov/books/NBK501371/ and https://www.e-lactancia.org/breastfeeding/domperidone/product/
Domperidone acts at the chemoreceptor trigger zone. It stimulates gastric emptying. It causes fewer central effects such as sedation and dystonia (although there are still reports of these) because it does not cross the blood–brain barrier as metoclopramide does. Its dopamine antagonist activity stimulates prolactin release, which makes it useful as a galactagogue (see section on drugs to increase lactation, pages 285–288). Domperidone is metabolised by cytochrome P450 so care should be taken with potential interactions. It is more than 90% bound to plasma proteins and has a low bioavailability on an empty stomach (15%) when taking orally due to first-pass hepatic and intestinal metabolism. Mean serum levels of domperidone measured in babies through maternal use of 10 mg three times daily was only 1.2 ng per millilitre. The total amount of the drug that would be ingested by the infant (Da Silva et al. 2001) would be extremely small (about 180 ng per kilogramme daily, assuming a daily milk intake of 150 ml per kilogramme). Relative infant dose quoted as 0.01– 0.04% (Hale 2017 online access). The BNF states that the amount secreted into breastmilk is probably too small to be harmful.
· Ondansetron (Zofran™)
This is an anti-emetic originally used to treat people who have severe sickness when being treated with chemotherapy for cancer. Ondansetron is frequently used for nausea during and after caesarean section, usually in doses of 4 to 8 mg intravenously. Use during and after caesarean section appears to not affect the onset of breastfeeding. No adverse infant effects have been reported or among women who received ondansetron postpartum in a pharmacokinetic study. Use of ondansetron in nursing mothers beyond the immediate postpartum setting has not been studied well, but the drug is licensed for use in infants as young as 1 month of age. See https://www.ncbi.nlm.nih.gov/books/NBK500798/ and https://www.e-lactancia.org/breastfeeding/ondansetron/product/
This drug is a 5-HT3 antagonist with antiemetic activity. It is also for the prevention and treatment of post-operative nausea and vomiting that have not responded to other antiemetic agents. Ondansetron may also be used for nausea in pregnancy. It is licenced for use in children It is 60% orally bio-available and 70–75% plasma protein bound. The terminal half-life is three hours after oral doses. There are no studies on transfer into breastmilk although it has been found in animal studies (BNF).
A large, well-designed study found that the vast majority of babies exposed to ondansetron in the womb (at least 998 out of every 1,000) are born without cleft lip and/or palate Ondansetron
Third Line
Corticosteroids
Corticosteroids are sometimes prescribed for women with hyperemesis gravidarum that has not responded to other treatments including rehydration together with anti-emetics. There is no strong evidence that use of corticosteroids in early pregnancy increases the chance of cleft lip and palate or heart defects in the baby. Use in pregnancy also does not appear to increase the chance of the baby having a low birth weight. Some studies have shown that pregnant women taking corticosteroids have a higher chance of preterm delivery. However, it is thought that this is likely caused by the underlying illnesses that steroids are commonly used to treat rather than a direct effect of steroids themselves. https://www.medicinesinpregnancy.org/Medicine–pregnancy/Corticosteroids—systemic/
Pregnancy Sickness Support in the UK found that many women seeking terminations in desperation had not been offered the full range of treatments available and fewer than 10% had been offered steroids
Other non-medical treatments
· Ginger
The conclusion from 6 randomised controlled trials with a total of 675 participants was that ginger extract at 1000 mgs per day may be effective treatment for NVP. However , the small number of patients in these studies allocated to receive ginger (n=303) may have been insufficient to properly test the safety of ginger with regards to pregnancy outcome. ( Viljoen, E., Visser, J., Koen, N. et al. A systematic review and meta-analysis of the effect and safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J 13, 20 (2014).) The authors found that Ginger did not significantly reduce the number of vomiting episodes during NVP, when compared to placebo, although there was a trend towards improvement. Many mothers have reported feeling angry and frustrated that this is recommended so frequently but that they found it caused side effects as well as not being effective. It is definitely not the answer to all NVP!
· Acupressure
Stimulation of the acupressure point, located three fingers breadth above the wrist, has been used for many years to treat nausea from a variety of causes. Mohd Nafiah et al (2022) concluded that the use of acupressure wristbands at the P6 point was also able to decrease the frequency of antiemetics and increase the rate of urine ketone clearance. The implication of the trial was the reported as the existence of an effective adjunct to alleviate the severity of nausea and vomiting in pregnant women with hyperemesis gravidarum, thereby improving their quality of life. There are no concerns about the safety of acupressure in pregnancy ( Mohd Nafiah, N.A.; Chieng, W.K.; Zainuddin, A.A.; Chew, K.T.; Kalok, A.; Abu, M.A.; Ng, B.K.; Mohamed Ismail, N.A.; Nur Azurah, A.G. Effect of Acupressure at P6 on Nausea and Vomiting in Women with Hyperemesis Gravidarum: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 10886.)
Conclusion
We should not underestimate how NVP and HG affect pregnant women. We should listen to how they are feeling and ask how we can help. Untreated symptoms can lead to lifetime mental health issues.
“I had morning sickness (not hyperemesis). The first 4 months I went from bed to the sofa, my husband did everything. I couldn’t look at food, walk into the kitchen to get a drink etc. I wasn’t physically that sick but the nausea was absolutely horrendous. Constantly, nothing stopping it, the minute I woke to the second I fell asleep for 4 months. I lost 6kg by my first scan. Although it got better I still felt slightly sick through the whole pregnancy. I was refused anti nausea meds by multiple doctors, even the midwife shrugged it off. The effect it has had on me even now (my daughter is 2.5) is horrible. I still can’t eat certain foods, put too much food in my mouth and the slightest nausea (which I get often due to anxiety, migraines etc) sends me into complete panic.”
“What would you like professionals to understand? The struggle and how debilitating it is.”
“Medically, only one doctor seemed to have any awareness of what I was suffering from. Others told me “I’d be better in a couple of weeks” every two weeks.”
Resources
Pregnancy Sickness Support https://www.pregnancysicknesssupport.org.uk/
RCOG Green Top Guidelines https://www.rcog.org.uk/guidance/browse-all-guidance/green-top-guidelines/the-management-of-nausea-and-vomiting-of-pregnancy-and-hyperemesis-gravidarum-green-top-guideline-no-69/
UKTIS Medicines in Pregnancy https://www.medicinesinpregnancy.org/About-Us/
