I know that this page is about breastfeeding and medication but I think that is important to share this too. I started writing it for another organisation a year ago but it hasnt gone anywhere so now it is here.
Anyone who is on sodium valproate (Epilim) should be taking adequate contraceptive protection
https://www.fsrh.org/news/mhra-contraception-drugs-birth-defects-fsrh-guidance/ .
It could be for epilepsy or it could be as a mood stabiliser but it is essential that you do not become pregnant. This factsheet explains why
In the UK valproate is licensed for use for epilepsy and bipolar disorder. The Medicines and
Healthcare Products Regulatory Agency (MHRA) regulates prescribing for the UK. Recent changes in
prescribing regulations (4) means that valproate must no longer be used in any woman or girl able to
have children unless there is no alternative and she has a pregnancy prevention programme (PPP) in
place. For details see reference 4. It is hoped that the increased regulation will lead to many less
children being born with Foetal valproate syndrome (10). It is imperative that any mother who is
taking valproate should be using good contraception.
Definition
Foetal valproate syndrome (FVS), results when a foetus is exposed to sodium valproate. It is
characterized by distinct facial abnormalities, congenital anomalies and developmental delay
(especially in language and communication). (1)
Incidence
FVS is a rare disease (defined as one that affects fewer than 200,000 people worldwide). Recent
evidence shows that the number of children born to mothers who took valproate during pregnancy
in 2017 in the UK is roughly 250 children (2, 3). There are also similar problems associated with
taking other anti-epileptic drugs, but they are less frequent and severe.
Signs and symptoms of FVS
Valproate is a highly teratogenic drug. Use in pregnancy leads to physical birth defects in 10 in every
100 babies (compared with a rate of 2 to 3 in 100 when mothers have not taken valproate) and
neurodevelopmental disorders in approximately 30 to 40 in every 100 children (4). The physical
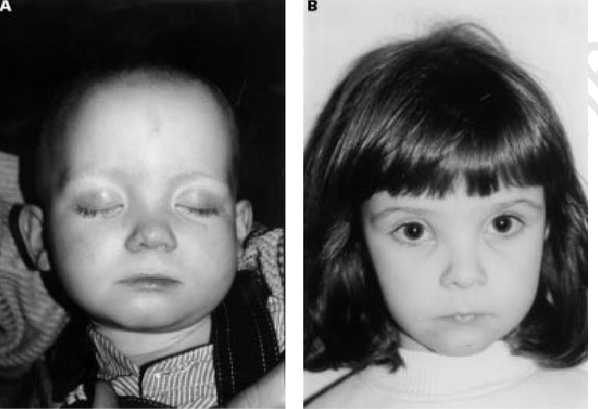
symptoms of FVS vary but may include characteristic facial features (see Figure 1)(5), spina bifida,
congenital heart defects, cleft lip and/or cleft palate, genital abnormalities, such as hypospadias and
skeletal abnormalities.
Figure 1 Children exposed to valproate alone. (A) A boy aged 22 months. Note epicanthic folds, infraorbital
grooves, long, shallow philtrum, and thin upper lip. (B) A girl aged 3 years 10 months, older sister of (A).
Note medial deficiency of eyebrows, infraorbital grooves, short nose with anteverted nares, long, shallow
philtrum, and thin upper lip. (C) A girl, aged 11 years 4 months. Note thin eyebrows, medial deficiency of
eyebrows, flattened nasal tip, shallow philtrum, and thin upper lip. (6).

The neural developmental disorders associated with valproate use in the mother during pregnancy
include:
● Delays in development such as talking and walking later, lower intellectual abilities, poor
language skills (speaking and understanding), and memory problems (6)
● The IQ in school-aged children (age 6 years old) is on average 7–10 points lower than
children exposed to other antiepileptic drugs (7)
● A 3-fold increased risk of autistic spectrum disorder and 5-fold increased risk of childhood
autism compared with the general population (8)
● Increased risk of attention deficit/hyperactivity disorder (ADHD) (9)
Investigations for FVS
There are no specific tests for FVS. The diagnosis is made by a pattern of physical, behavioural and
cognitive problems in a child who has been exposed to valproate during pregnancy. The diagnosis
usually needs to be made by an appropriately trained paediatrician. There is no automatic follow up
pathway for exposed babies. If no abnormalities are obvious at birth the baby is usually discharged
with instructions to be referred back if problems develop. However neurodevelopmental issues may
be subtle and overlooked by generalist healthcare professionals. In addition, some
neurodevelopmental issues, especially if mild, cannot be diagnosed until much later in childhood, at
which point maternal medication history in pregnancy may either not be available or not considered.
Universal follow up has been recommended (10) for all babies exposed to valproate, but this is not
yet available.
Treatment
Although there is no treatment for FVS, early diagnosis and support can make a massive difference
for the child and their family. Many of these children should qualify for special educational needs
and disability services (SENDs), but unless they are identified and referred for detailed assessment
they will not receive additional services.
Any harm to babies exposed in utero can be documented on a Yellow Card or women can self-refer
to the UK Epilepsy and Pregnancy Register
Patient support groups
Epilepsy Action: www.epilepsysociety.org.uk/
Epilepsy Society: www.epilepsysociety.org.uk/
FACSaware: www.facsaware.net/
References
- Orphanet Definition of Foetal Valproate Syndrome https://www.orpha.net/consor/cgi
bin/OC_Exp.php?Lng=GB&Expert=1906. - Gov.UK. Valproate medicines: are you acting in compliance with the pregnancy prevention
measures? https://www.gov.uk/drug-safety-update/valproate-medicines-are-you-in-acting
in-compliance-with-the-pregnancy-prevention-measures. - Medicines and Healthcare Products Regulatory Agency. CPRD study monitoring the use of
valproate in girls and women in the UK: January 2010 to June 2018
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_
data/file/765558/CPRD-valproate-usage-17122018.pdf - Medicines and Healthcare Products Regulatory Agency Valproate use by women and girls
Information about the risks of taking valproate medicines during pregnancy.
https://www.gov.uk/guidance/valproate-use-by-women-and-girls
https://assets.publishing.service.gov.uk/media/54bd3a23e5274a15b3000009/Valproate_bookle
t_for_patients_Jan_2015.pdf - S J Moore, P Turnpenny, A Quinn et al, A clinical study of 57 children with foetal
anticonvulsant syndromes J Med Genet 2000;37:489–497 - Bromley RL, Mawer G, Love J, Kelly J, Purdy L, McEwan L. Early cognitive development in
children born to women with epilepsy: a prospective report Epilepsia 2010; 51: 2058 - https://doi.org/10.1111/j.1528-1167.2010.02668.x.
- Meador, KJ, Baker, GA, Browning N, Cohen MJ, Bromley RL., Clayton-Smith J, Kalayjian LA,
Kanner A, Liporace, JA, Pennell PB, Privitera M, Loring D, for the NEAD Study Group (2013).
Foetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD study): a
prospective observational study. Lancet Neurology, 12(3), 244-252 - Christensen J et al. Prenatal valproate exposure and risk of autism spectrum disorders and
childhood autism. JAMA 2013; 309: 1696-1703.
https://jamanetwork.com/journals/jama/fullarticle/1681408 - Cohen MJ et al. Fetal antiepileptic drug exposure: motor, adaptive and emotional/
behavioural functioning at age 3 years. Epilepsy Behav 2011; 22: 240 - https://www.epilepsybehavior.com/article/S1525-5050(11)00359-3/fulltext.
- Shakespeare J, Sisodiya S. (2019) Guidance document on valproate use in women and girls of
childbearing years. https://www.rcgp.org.uk/about-us/news/2019/march/thirteen-uk - healthcare-bodies-launch-pragmatic-guidance-on-valproate-use.aspx