After some discussions with the Thyroid Trust I have put this information together
PDF of this factsheet available here https://breastfeeding-and-medication.co.uk/wp-content/uploads/2023/02/thyroid-and-breastfeeding-.pdf
Underactive Thyroid and Breastfeeding (Hypothyroid)
“Many medical professionals seem unaware of how important adjusting meds during and post pregnancy is and that it can influence breastfeeding as well”
Description
An underactive thyroid gland is where the thyroid gland does not produce enough hormones. Common signs of an underactive thyroid are :
- tiredness,
- weight gain
- feeling depressed
- being sensitive to the cold,
- slowed thought processes,
- muscle pains
- dry skin and brittle hair.
Most people presenting with symptoms of depression will be asked to have a blood test before medical treatment. Similarly although it is normal to lose the thicker hair which is enjoyed in pregnancy, significant hair loss should also be considered a possible symptom.
Hypothyroidism is identified by blood tests which are conducted regularly until they are within stabilised levels. Blood levels are ideally taken routinely after delivery and especially if the mother reports a poor milk supply. Levels at the low end of normal are frequently associated with low prolactin and poor breastmilk supply.
Hypothyroidism is ten times more common in women than it is in men. In the UK, around 1-2 in 100 people have hypothyroidism. It most commonly develops in adult women and becomes more common with increasing age. However, it can occur at any age and can affect anyone.
Treatment
Levothyroxine is secreted in extremely low levels into breastmilk, if at all (Bennett 1988; Oberkotter 1983; Sato 1979). It is highly bound to proteins in the maternal plasma, so little is free to pass into breastmilk.
The level to which the baby will be exposed via breastmilk is virtually undetectable. Levels secreted into milk are too low to influence tests for neonatal hypothyroidism according to Martindale (2017). There is no need to routinely test breastfed babies unless there They should be swallowed with water on an empty stomach, with no food for 30 minutes afterwards.
References
- Bennett PN (ed.), Drugs and Human Lactation, Amsterdam: Elsevier, 1988.
- Brown A Jones W A guide to breastfeeding for the medical professional Routledge 2019
- Drugs and Lactation Database (LactMed®) https://www.ncbi.nlm.nih.gov/books/NBK501003/
- E lactancia https://www.e-lactancia.org/breastfeeding/levothyroxine/product/
- Jones W Breastfeeding and Medication Routledge 2018
- Martindale The Complete Drug Reference. Pharmaceutical Press 2017
- Oberkotter LV, Tenore A, Separation and radioimmunoassay of T3 and T4 in human breastmilk, Horm Res, 1983;17:11–18.
- Sato T, Suzuki Y, Presence of triiodothyronine, no detectable thyroxine and reverse triiodothyronine in human milk, Endocrinol Jpn, 1979;26:507–13.
Overactive thyroid and breastfeeding (Hyperthyroid disease)
“I was told to stop breast feeding immediately after being put on carbimazole for an overactive thyroid. I’m still so angry that it wasn’t necessary”
Description
Hyperthyroidism has a variety of causes. It is ten times more common in women than men, and typically begins between 20 and 40 years of age It is often diagnosed post-partum in breastfeeding women.
Symptoms include:
- nervousness,
- anxiety and irritability,
- mood swings,
- difficulty sleeping,
- persistent tiredness and weakness,
- sensitivity to heat, palpitations,
- weight loss (despite increased appetite),
Three in every 4 cases of hyperthyroid are caused by Graves’ disease, an auto-immune condition. Less commonly it develops because of nodules on the thyroid gland.
Treatment
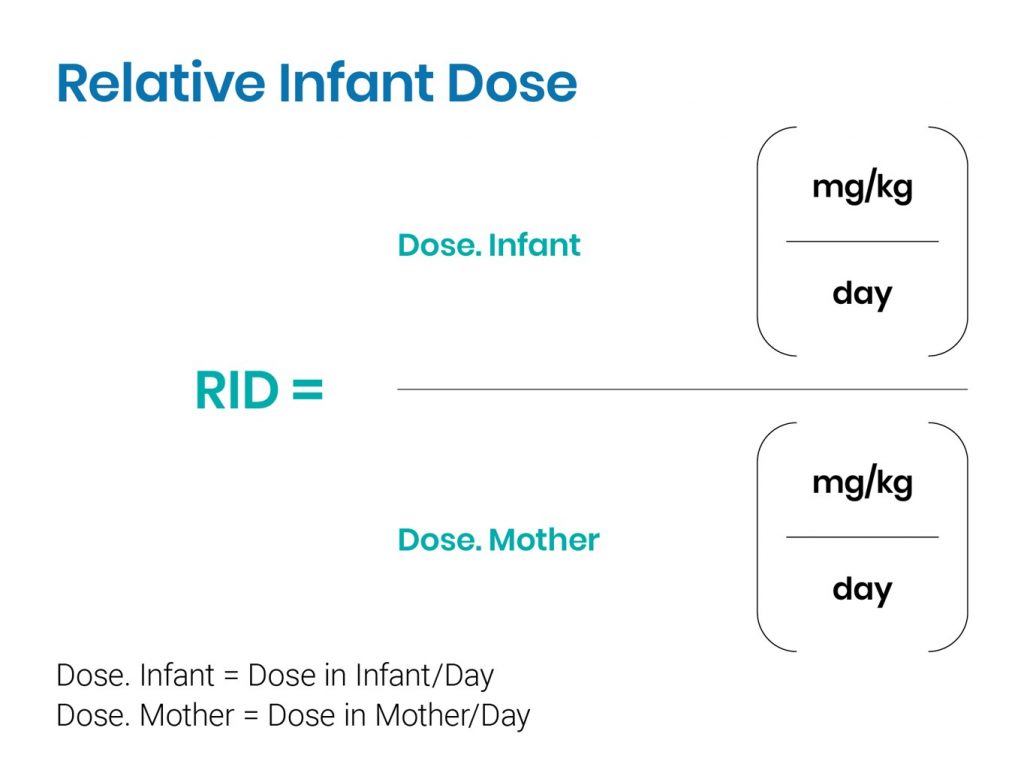
Carbimazole – is a pro-drug that is bioactivated to methimazole. It produces sub-clinical levels in infants exposed to less than 30 mg a day through their mother’s breastmilk (Rylance 1987). Carbimazole has a relative infant dose of 2.3% – 5.3% (Hale) where levels less than 10% are regarded as compatible with breastfeeding.
In a study of 5 five lactating women receiving 40 mg/d, the mean concentration of methimazole in milk measured by .Johansen was 182 µg/L, with a mean milk/serum ratio of 0.98. The mean total amount of methimazole excreted in milk over 8 h was 34 µg. The limited data suggest that the transfer of carbimazole is too low to affect thyroid function in breastfeeding infants.
If the drug is used at a dose above 30mg, monitoring of the infant’s thyroid function periodically might be advisable. Otherwise monitoring would only be necessary if the baby exhibits clinical symptoms.
In February 2019 the MHRA issued a notice that “ Carbimazole is associated with an increased risk of congenital malformations, especially when administered in the first trimester of pregnancy and at high doses. Women of childbearing potential should use effective contraception during treatment with carbimazole.” https://breastfeeding-and-medication.co.uk/fact-sheet/carbimazole-in-women-of-childbearing-age
References
- Brown A Jones W A guide to breastfeeding for the medical professional Routledge 2019
- Drugs and Lactation Database (LactMed®) https://www.ncbi.nlm.nih.gov/books/NBK501759/
- E lactancia https://www.e-lactancia.org/breastfeeding/carbimazole/product/
- Hale TW and Krutsch K Hale’s Medications & Mothers’ Milk™ 2023: A Manual of Lactational Pharmacology (also available as https://www.halesmeds.com/ by subscription). Springer Pub
- Jones W Breastfeeding and Medication Routledge 2018
- MHRA Carbimazole: increased risk of congenital malformations; strengthened advice on contraception www.gov.uk/drug-safety-update/carbimazole-increased-risk-of-congenital-malformations-strengthened-advice-on-contraception
- Rylance GW, Woods CG, Donnelly MC, Oliver JS, Alexander WD, Carbimazole and breastfeeding, The Lancet, 1987;1(8538):928
Propylthiouracil has been the drug of choice in a breastfeeding mother as the transfer into breastmilk is lower than that with carbimazole. In 2009 the US Food and Drug Administration (FDA) in the USA alerted practitioners to an increased risk of hepatotoxicity (liver toxicity) with PTU use and recommended that all patients should be observed and monitored for signs of liver disease, particularly during the first six months of treatment. Signs of liver damage, which should be reported to the prescriber immediately are anorexia, nausea, vomiting, fatigue, abdominal pain, jaundice, dark urine, or pruritus (BNF). Propylthiouracil crosses the placenta and in high doses may cause foetal goitre and hypothyroidism.
Only small amounts of propylthiouracil are secreted into breastmilk and reports suggest that levels are too low to produce side effects (Cooper 1987). Propylthiouracil is extensively plasma protein bound (80%) and has an oral bioavailability of 50–75% which is low. At doses of 400 mg, a study of nine women and their babies showed levels of PTU in milk reached only 0.7 µg per millilitre (Kampmann 1980). One of the babies was studied for five months during which the mother received 200–300 mg of PTU daily. There were no changes to the infant’s thyroid functions. Momotani’s (2000) study of 11 babies has shown that up to 750 mg produced no changes in babies monitored up until 11 months of age. Monitoring is recommended as a precaution if clinical symptoms are identified in the baby.
References
- Cooper DS, Antithyroid drugs: to breastfeed or not to breastfeed, Am J Obstet Gynecol, 1987;157:234–5.
- Drugs and Lactation Database (LactMed®) https://www.ncbi.nlm.nih.gov/books/NBK501084/
- E lactancia https://www.e-lactancia.org/breastfeeding/propylthiouracil-ptu/product/
- FDA Alert 2009, Information for Healthcare Professionals – Propylthiouracil-Induced Liver Failure (www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm162701.htme).
- Hale TW and Krutsch K Hale’s Medications & Mothers’ Milk™ 2023: A Manual of Lactational Pharmacology (also available as https://www.halesmeds.com/ by subscription). Springer Pub
- Jones W Breastfeeding and Medication Routledge 2018
- Kampmann JP, Johansen K, Hansen JM, Helweg J, Propylthiouracil in human milk, The Lancet,1980;1(8171):736–7.
- Momotani N, Yamashita R, Makino F, Noh JY, Ishikawa N, Ito K, Thyroid function in wholly breastfeeding infants whose mothers take high doses of propylthiouracil, Clin Endocrinol (Oxf), 2000;53(2):177–81.
Propranolol is often used to relieve symptoms of an over active thyroid. It is 90% plasma protein bound, the milk plasma ratio and it is only 30% orally bio available. Its relative infant dose is 0.3-0.5% so virtually none passes into milk and breastfeeding can continue as normal. This has been confirmed in several studies.
References
- Bauer JH, Pape B, Zajicek J, Groshong T. Propranolol in human plasma and breast milk. Am J Cardiol. 1979; 43(4):860-862.
- Brown A Jones W A guide to breastfeeding for the medical professional Routledge 2019
- Drugs and Lactation Database (LactMed®) https://www.ncbi.nlm.nih.gov/books/NBK501162/
- Elactancia https://www.e-lactancia.org/breastfeeding/propranolol/product/
- Hale TW and Krutsch K Hale’s Medications & Mothers’ Milk™ 2023: A Manual of Lactational Pharmacology (also available as https://www.halesmeds.com/ by subscription). Springer Pub
- Jones W Breastfeeding and Medication Routledge 2018
- Lewis AM, Patel L, Johnston A, Turner P. Mexiletine in human blood and breast milk. Postgrad Med J. 1981 Sep;57(671):546-547.
- Smith MT, Livingstone I, Hooper WD, Eadie MJ, Triggs EJ. Propranolol, propranolol glucuronide, and naphthoxylactic acid in breast milk and plasma. Ther Drug Monit. 1983; 5(1):87-93.
- Taylor EA, Turner P. Anti-hypertensive therapy with propranolol during pregnancy and lactation. Postgrad Med J. 1981;57(669):427-430.
Radiotherapy involving ingestion of iodine is not suitable during breastfeeding as iodine concentrates in breastmilk and lasts for some time so would mean stopping breastfeeding