Although we now try very hard to avoid prescribing antibiotics unless essential ( because of the risk that in the future we wont have antibiotics which are as effective against all infections), sometimes they are necessary. The use of antibiotics during breastfeeding often causes disquiet because most of them cause the baby to have loose bowel motions, sometimes tummy cramps, and sometimes vomiting. Is continuing to breastfeed actually causing harm and should feeding be interrupted? Do we need pre-biotics and probiotics to redress the balance in the baby’s gut?
It is hard to watch a baby in distress but it is important to remember that when we breastfeed during an infection we are also passing antibodies to that infection in breastmilk to protect the baby. Breastmilk contains all the factors to redress the balance and return the baby’s gut to its normal state far better than any probiotics derived from other sources, in my opinion.
But the ultimate choice is that of the breastfeeding mother.
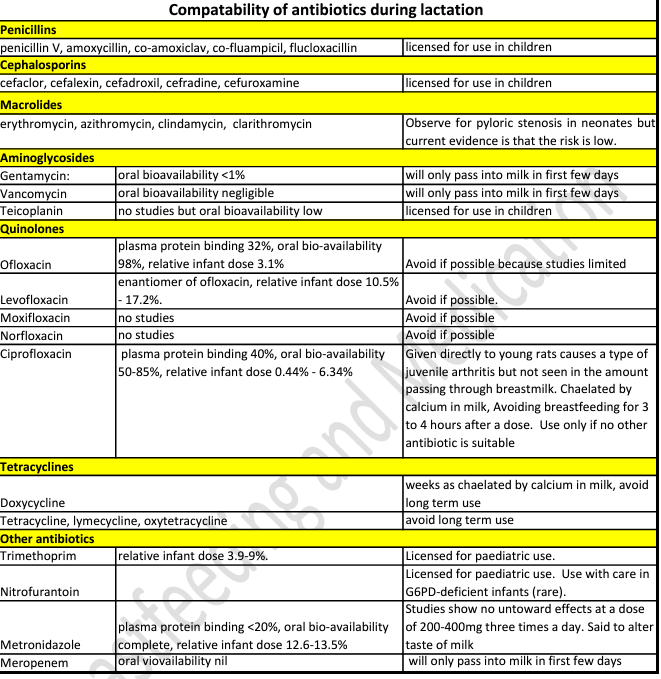
January 2024 the MHRA issued guidance on fluoroquinolones : ” that fluoroquinolone antibiotics given systemically (by mouth, injection, or inhalation) must only be administered when no other antibiotics are appropriate for use, the Medicines and Healthcare products Regulatory Agency (MHRA) has announced. This means that fluoroquinolones should only be prescribed when other recommended antibiotics have failed, will not work due to resistance, or are unsafe to use in an individual patient.” https://www.gov.uk/government/news/mhra-introduces-new-restrictions-for-fluoroquinolone-antibiotics
Fluoroquinolone include ciprofloxacin, levofloxacin, moxifloxacin, and ofloxacin. If prescribed these as a first option please discuss with your prescriber. The MHRA guidance refers to use in adults only where no other antibiotic is available.
See also https://www.sps.nhs.uk/articles/using-metronidazole-during-breastfeeding
Metronidazole can be used during breastfeeding for most usual treatment courses. Recommendations apply to full term, healthy infants.
I hope that the information in this factsheet helps make that decision. Please email me if you want to discuss anything : wendy@breastfeeding-and-medication.co.uk
Antibiotics and breastfeeding factsheet pdf
Antibiotics are acknowledged to be overused which is one of the reasons that Multiple Resistant Staphylococcus aureus (MRSA) and Clostridium difficile have become more widespread. It is sensible to consider whether a mother needs to be treated with antibiotics before exposing both her and her breastfed baby. Babies exposed to antibiotics via their mother’s breastmilk may develop symptoms of colic, abdominal discomfort and diarrhoea. These are an inconvenience and not a reason to suspend breastfeeding. Research undertaken in Canada in 1993 (Ito et al. 1993) showed that 15% of women prescribed antibiotics chose not to take the medicine and continue to breastfeed, rather than expose their baby to a risk which they had been assured was minimal. By contrast, 7% stopped breastfeeding during therapy despite reassurance. The research team also examined the reporting of adverse effects by mothers made aware of potential diarrhoea in the child with antibiotics passing through breastmilk. Although more women warned of side effects reported clinical effects which they had noted and judged to be due to the medication, than those not made aware, the difference is not statistically significant (87% compared with 68%). No difference in compliance with the antibiotic regimen or breastfeeding pattern, were noted between the two groups (Taddio et al. 1995).
These follow recommendations from the doctor that the ‘infection’ may be self-limiting but if symptoms develop further or fail to resolve in the following 48 hours, then the course of antibiotics should be taken. Little et al. have suggested restricting the use in the treatment of otitis media, upper respiratory infection and sore throat ((Little 2002; 2005; 1997) beginning the public health message about reducing the use of antibiotics. It may also be useful in the management of mastitis.
References
• Abdellatif M e, Ghozy S, Kamel MG, Elawady SS Ghorab MMEAttia AW, Le Huyen TT, Duy DTVHirayama K, Huy NT. Association between exposure to macrolides and the development of infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis. Eur J Pediatr. 2019 178(3):301-314.
• Hale T. Hale’s medications & mothers’ milk. 19th ed. New York, USA: : Springer Publishing 2021. • Ito S, Koren G, Einarson TR, Maternal non compliance with antibiotics during breastfeeding, Ann Pharmacother, 1993;27(1):40–42.
• Ito S, Koren G, Einarson TR. Maternal Noncompliance with Antibiotics during Breastfeeding. Ann Pharmacother 1993;27:40–2. doi:10.1177/106002809302700110 • Jones W Breastfeeding and Medication Routledge 2018
• Jones W How to advise women on the safe use of medicines while breastfeeding The Pharmaceutical Journal, PJ, 2021, 306 (7949) https://pharmaceuticaljournal.com/article/ld/how-to-advise-women-on-the-safe-use-of-medicines-whilebreastfeeding
• LactMed https://www.ncbi.nlm.nih.gov/books/NBK501922/ • Little P, Delayed prescribing of antibiotics for upper respiratory tract infection, BMJ, 2005;331(7512):301.
• Little P, Gould C, Moore M, Warner G, Dunleavey J, Williamson I, Predictors of poor outcome and benefits from antibiotics in children with acute otitis media: pragmatic randomised trial, BMJ, 2002;325(7354):22
• Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth AL, Open randomised trial of prescribing strategies in managing sore throat, BMJ, 1997;314:722.
• Taddio A, Ito S, Einarson TR, Leeder JS, Koren G, Effect of counselling on maternal reporting of adverse effects in nursing infants exposed to antibiotics through breastmilk, Reprod
See also https://www.sps.nhs.uk/articles/using-tetracycline-antibiotics-during-breastfeeding
https://www.sps.nhs.uk/articles/using-macrolide-antibiotics-during-breastfeeding
https://www.sps.nhs.uk/articles/treating-impetigo-topically-during-breastfeeding