Home » GP information
Category Archives: GP information
Pain relief when breastfeeding
It is not acceptable to leave any mother in pain because she is breastfeeding nor to suggest that she could have more effective pain relief if she stopped breastfeeding.
I’m often asked about the safety of opioids during breastfeeding so this is a really interesting study
Despite opioids being used first line in emergency settings to treat severe acute extremity pain, there is limited evidence available to inform this practice.
In a study in JAMA (7 November 2017), researchers randomly assigned 416 patients in the emergency department with moderate-to-severe acute extremity pain to one of the following groups: 400mg ibuprofen/1000mg paracetamol; 5mg oxycodone/325mg paracetamol; 5mg hydrocodone/300mg paracetamol; or 30mg codeine/300mg paracetamol[1].
https://jamanetwork.com/journals/jama/article-abstract/2661581?redirect=true
I have written this powerpoint presentation which I hope explains the analgesic ladder and helps professionals to understand the compatibility of analgesics and breastfeeding
- Paracetamol or NSAID
- Paracetamol + NSAID
-
Paracetamol+NSAID+Opioid (at the lowest possible dose for the shortest possible time co prescribed with a laxative)
Non steroidal anti inflammatory drugs
- Compatible with breastfeeding: ibuprofen, diclofenac (Voltarol ™, Difene™), naproxen (Naprosyn™) https://breastfeeding-and-medication.co.uk/fact-sheet/naproxen-and-breastfeeding
- No data on compatibility with breastfeeding: etoricoxin (Arcoxia™), meloxicam (Mobic™)
- See https://www.sps.nhs.uk/articles/using-nsaids-during-breastfeeding
Opioids
- compatible with breastfeeding: oral morphine, dihydrocodeine
- https://breastfeeding-and-medication.co.uk/fact-sheet/dihydrocodeine-and-breastfeeding
- use with caution as may cause drowsiness: oxycodone (Oxycontin™, Oxyfast™)
- avoid if possible as may cause drowsiness: codeine
https://breastfeeding-and-medication.co.uk/thoughts/breastfeeding-and-codeine
https://breastfeeding-and-medication.co.uk/fact-sheet/accidental-dose-of-codeine-when-breastfeeding
All opioids can cause nausea and dizziness but almost invariably cause constipation so it is wise to commence stool softeners like lactulose and/or docusate both of which are compatible with breastfeeding as they don’t pass into milk.
See
https://breastfeeding-and-medication.co.uk/fact-sheet/constipation-laxatives-and-breastfeeding
Analgesics and breastfeeding Powerpoint


see also https://www.breastfeedingnetwork.org.uk/factsheet/analgesics/
https://breastfeeding-and-medication.co.uk/fact-sheet/dihydrocodeine-and-breastfeeding
https://breastfeeding-and-medication.co.uk/thoughts/breastfeeding-and-codeine
https://breastfeeding-and-medication.co.uk/fact-sheet/migraine-treatment-and-breastfeeding
Hypertension (raised blood pressure) and Breastfeeding
Many mothers experience raised blood pressure it seems. Is this due to our busy lifestyles, more mums giving birth at an older age? Who knows but it causes a lot of confusion. The drug normally initiated if a mother has symptoms of pre-eclampsia is labetolol. It is usually continued after delivery until the BP has settled. Virtually none passes into breastmilk. However, some mothers with poor circulation may notice sore, white nipples where the supply to the tip is decreased . If this happens the drug may need to be changed. Prolonged high BP in pregnancy can lead to restricted growth of the baby who may be born sleepy. Rather than just monitoring blood glucose levels the baby should be helped to attach to the breast and feed regularly or be given colostrum by spoon or syringe. A drop of colostrum can work magic.
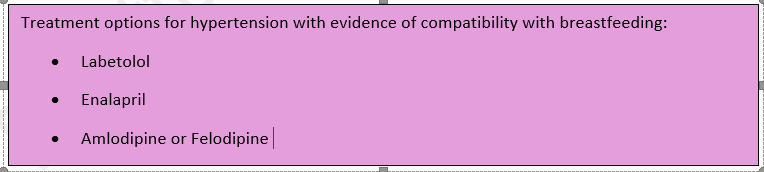
Later blood pressure rises can be treated with enalapril, amlodipine and felodipine which are all compatible with breastfeeding according to expert sources. The NICE Guidelines NG 133 (2019) can also guide good practice.
The data for this fact sheet is taken from my book Breastfeeding and Medication which provides more detail and references to studies. Please consider buying a copy for future reference.
There is much information in this factsheet.
Hypertension (raised blood pressure) is defined as sustained blood pressure above 140/90. Diet, obesity, heredity, race and stress all impact on blood pressure. High cholesterol, high salt content in the diet and saturated fat intake increases the long-term health risk.
Breastfeeding women may have had a previous event which presents a challenge to pregnancy and lactation e.g., stroke, heart attack, renal complications, SVT etc. In the past these might have produced barriers to childbirth but now seem to be so well controlled mothers are able to give birth and look after their own health.
There are several types of drugs used to treat hypertension some of which we have no data on with respect to use in breastfeeding mother, others should be avoided where possible.
For more details and references see Breastfeeding and Medication Jones W Routledge 2018
Diuretics
All diuretics should be avoided unless essential for health of the mother. By removing excess fluid from the body diuretics may reduce milk supply. This is more likely with furosemide than Bendroflumethiazide or bumetanide, but this category of drugs should be avoided during lactation to control blood pressure but only fluid retention, where essential
Bendroflumethiazide – unknown effect from low dose 2.5mg daily
Indapamide – No information is available on the amount of indapamide in breastmilk. Intense diuresis with large doses may decrease breastmilk production.
Furosemide – more likely to reduce supply due to intense diuresis
Bumetanide – low risk in established supply
Spironolactone – an aldosterone receptor antagonist used as a diuretic in various conditions associated with oedema, as well as in the treatment of hypertension. Its value is in sparing potassium loss. It is metabolised to canrenone which was found in the breastmilk of one mother taking 25mg four times a day by Phelps (1977). He suggested the amount absorbed by the baby would be 0.2% of the mother’s daily dose. Spironolactone is 90% plasma protein bound and has a bioavailability of 90% (Martindale 2017) 70% (Hale 2017). The American Academy of Paediatrics considers it compatible with breastfeeding. The BNF states that although its metabolite is present in milk, the amount is probably too small to be harmful.
ACE inhibitors
This family of drugs are potentially teratogenic but can be used during lactation
Enalapril. This is the ACE with most evidence of safety during lactation. Redman et al. (1990) studied five women taking 20 mg enalapril, it was not detectable after 4 hours in four of the five women while the average peak level of enalaprilat (the metabolite of enalapril) was 1.7 µg per litre. No adverse events were reported in four babies exposed to maternal levels of 5–10 mg. Huttenen et al. (1989) studied three women after single doses of enalapril up to 10 mg. Enalaprilat levels were not detected and the concentration of ACE activity in milk was unchanged. Rush et al. (1989) deduced that the total amount of enalapril and its metabolite to which a baby would be exposed was 2 µg of enalaprat while unlicensed use of enalapril from 1 month (BNFC) is 100 µg per kilogramme per day. Relative infant dose quoted as 0.2% (Hale 2017 online access).
BNF data recommend that the drug is avoided in the first few weeks after delivery due to the risk of profound neonatal hypotension; it can be used in older infants if essential but recommends that the infant’s blood pressure is monitored.
Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Captopril: Devlin and Fleiss’ study (1981) of 12 women showed that the concentration of captopril in breastmilk was about 1% of maternal plasma, equivalent to 4.7 µg per litre in breastmilk of mothers taking 300 mg daily and no adverse effects were noted in the babies. Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Ramipril: No data are available on transfer into breastmilk. Ramipril has an active metabolite ramiprilat, which is approximately 56% plasma protein bound.
Lisinopril: There is no information on the transfer of lisinopril into breastmilk, although the oral bioavailability is only 29%. It is not significantly bound to plasma proteins.
Perindopril: There are no data available on the transfer of perindopril into breastmilk. It is metabolised to perindoprilat which is the active drug. Plasma protein binding is reported to be 10–20% and oral bioavailability is 65–75%.
Quinapril: rapidly converted to its active metabolite quinaprilat. Begg studied 6 women taking 20mg quinapril daily. Four hours after the dose no drug was recovered from milk. No Quinaprilat was detected at any time. The authors therefor suggested that quinapril is safe in breastfeeding.
Beta blockers
Beta blocker of choice in a mother during breastfeeding based on evidence of benefit and safety for the baby is Metoprolol, propranolol or labetolol
In many maternity units the use of beta blockers triggers the hypoglycaemia policy involving blood sugar testing. The amount of labetolol, propranolol and metoprolol passing into breastmilk is low and these drugs are less likely to lower blood sugars than atenolol (which has low plasma protein binding and passes more extensively into milk). The risk to the baby stems from the fact that babies born to mothers with pre-eclampsia may be born (or induced) early or may have experienced intra-uterine growth retardation. The efficacy of the baby’s feeding and milk transfer should be assessed as well as blood sugars. If necessary, the mother may need to hand express and syringe/cup/spoon feed colostrum to her infant.
Atenolol: diffuses into breastmilk in concentrations similar to or higher than those in maternal blood demonstrated by m/p ratios of 1.5–6.8. Despite this, the authors calculated the infant would only be exposed to 0.13 mg per day following a maternal dose of 50 mg per day (Liedholm 1983). Cyanosis and bradycardia in a 5-day-old term infant associated with maternal intake of 50 mg atenolol twice daily in breastmilk has been reported. The infant recovered when breastfeeding was interrupted (Schimmel et al. 1989). Other authors have reported no adverse effects in 15 infants aged 3 days to 2 weeks exposed to 50–100 mg atenolol (Bhamra et al. 1983; White et al. 1984; Kulas et al. 1984). It is not licensed for use in children under the age of 12 years. Relative infant dose quoted as 6.6% (Hale 2017 online access).
Atenolol has low plasma protein binding and therefore passes more freely into breastmilk. Caution is particularly advised in neonates because of the renal excretion of this drug.
Labetolol; Michael’s study of 25 patients (1979) taking between 330 and 800 mg labetolol daily showed a m/p ratio less than 1, although one patient taking 1200 mg daily produced milk samples where the concentration in milk exceeded that in maternal plasma. Lunell et al.’s study (1985) produced similar results. However, no baby in these studies exhibited any adverse drug reactions. Mirpuri et al. (2008) reported that a 26-week premature baby exhibited bradycardia and premature beats when tube fed expressed breastmilk from its mother who was receiving 300 mg labetolol twice daily. Its condition returned to normal when formula milk was substituted. McGuinness identified that a mother’s intake of labetolol had triggered symptoms of Raynaud’s syndrome due to restriction of blood flow to the extremities. This should be borne in mind with any mum reporting panful breastfeeding when on beta blockers.
Metoprolol: Studies have shown that metoprolol also produces m/p ratios in excess of 1 (Sandström and Regårdh 1980; Liedholm et al. 1981). However, the absolute level of drug transferring to the baby is small and studies have failed to detect metoprolol at significant levels in infant plasma (Kuklas et al. 1984). Although the drug is well-absorbed, it undergoes extensive first-pass metabolism. No adverse events have been reported in babies exposed to metoprolol via breastmilk (Ho et al. 1999; Lindeberg et al. 1984
Bisoprolol: Only one study of the use of bisoprolol appears in the literature. Khurana studied a mother who was initiated on it 6 days after birth for a cardiac condition. She expressed samples of milk on day 11 and 18 after birth. Drug levels in milk were undetectable but the baby did not receive any breastmilk, so data is incomplete. See https://breastfeeding-and-medication.co.uk/fact-sheet/bisoprolol-and-breastfeeding
Propranolol: almost completely absorbed from the gastrointestinal tract but undergoes first-pass metabolism. It is highly lipid soluble and is approximately 90% plasma protein bound. It has at least one active metabolite but the impact of this is unclear.
In adults it may be used to lower blood pressure, to relieve symptoms of hyperthyroidism, to prevent migraines or to prevent panic attacks. See https://breastfeeding-and-medication.co.uk/thoughts/propranolol-and-breastfeeding
In a study of three women (Smith 1983) it was calculated that the maximum dose likely to be ingested by a breastfed infant would be less than 0.1% of the maternal dose.
Angiotensin II receptor antagonists
This group of drugs is given to patients who are unable to tolerate ACE inhibitors to treat hypertension and heart failure. As with ACE inhibitors, this group of drugs is contra-indicated in pregnancy. There are few data on transfer into breastmilk and the use of ACE inhibitors is recommended. This class of drug might be expected to produce low levels in breastmilk because of the high protein binding and low bioavailability but no data exist to support this assumption.
Candestartan : has limited oral bio availability of 14%, and a plasma protein binding > 99%. There is one study of 3 breastfeeding mothers, all stabilized on candesartan (8-32 mg daily ). They provided milk and plasma samples over 24 hours. Plasma samples were obtained from 2 of the babies The relative infant dose was estimated to be 0.09%. Candesartan was undetectable (less than 0.2 micrograms/L) in infant plasma samples (Coberger 2019, LactMed).
Irbesartan; oral bio availability 60-80% and plasma protein binding 90%. Because no information is available on the use of irbesartan during breastfeeding it is best avoided. If a sartan is considered essential candesartan might be preferable
Losartan; oral bio availability of 33%, and high plasma protein binding of 99.8%. Kearney (2018) suggests that the high protein-binding of losartan and low oral bioavailability makes excretion into breast milk and subsequent absorption by the baby unlikely. She suggests that if the mother has developed Postpartum cardiomyopathy, breastfeeding need not be discouraged. However, there are no relevant published data on excretion into breast milk.
Valsartan; has an oral bio availability 23%, and plasma protein binding of 95%. There are no relevant published data on excretion into breast milk. Candesartan may be seen as the best option if a sartan is considered essential.
Calcium channel blockers
Nifedipine: relaxes vascular smooth muscle and dilates coronary and peripheral arteries. It has activity in reducing blood pressure and in the treatment of Reynaud’s syndrome. Nifedipine is almost completely absorbed from the GI tract but undergoes extensive first-pass metabolism. Side effects for the mother include flushing and headache, which may limit its usefulness. It is present in breastmilk but in levels too small to be harmful and there have been no reports of adverse effects in babies. See https://breastfeeding-and-medication.co.uk/fact-sheet/february-is-raynaud-s-awareness-month-www-sruk-co-uk
Amlodipine: A study of 31 postpartum women (Naito 2015) with pregnancy-induced hypertension received amlodipine 5 mg daily by mouth, with the dosage increased as needed to maintain blood pressure of 140/90 mm Hg or less (mean dosage for the group was 6 mg daily. Maternal blood and breastmilk samples were obtained after at least 6 days of therapy. The median milk concentration was 11.5 µg/L, and no infant showed any adverse effects.
Felodipine: Small amounts of felodipine may get into breast milk, but it’s not known if this is harmful to the baby (BNF). Oral bio availability 20%, plasma protein binding >99%, no studies of passage into breastmilk have been located
Diltiazem: Diltiazem is used for its antiarrhythmic, anti-anginal and antihypertensive properties but rarely in women of childbearing age unless there are very specific indications from the medical history. It is rarely used simply to treat hypertension.
Alpha blockers
Avoid unless essential to mother’s health. This class of drugs are generally only used in addition to other drugs with poorly controlled blood pressure. They are not normally used as first line or monotherapy
Doxazosin: Jensen published a paper on one mother breastfeeding a 6-month-old. She received 4 mg daily for 2 days. The maximum milk concentrations were 2.9 and 4.2 µg/L. This drug should only be used in extreme circumstances and with close monitoring of the infant, for drowsiness, poor feeding, low blood pressure.
Terazosin: no studies in breastfeeding. Terazosin has rather powerful effects on the prostate and testes producing testicular atrophy in some animal studies (particularly new-born) and is therefore not preferred in pregnant or in lactating women (Hale)
NICE Guidance NG 133 (June 2019)
1.9 Antihypertensive treatment during the postnatal period, including during breastfeeding
1.9.1 Advise women with hypertension who wish to breastfeed that their treatment can be adapted to accommodate breastfeeding, and that the need to take antihypertensive medication does not prevent them from breastfeeding. [2019]
1.9.2 Explain to women with hypertension who wish to breastfeed that:
- antihypertensive medicines can pass into breast milk
- most antihypertensive medicines taken while breastfeeding only lead to very low levels in breast milk, so the amounts taken in by babies are very small and would be unlikely to have any clinical effect
- most medicines are not tested in pregnant or breastfeeding women, so disclaimers in the manufacturer’s information are not because of any specific safety concerns or evidence of harm.
- Make decisions on treatment together with the woman, based on her preferences. [2019]
1.9.3 As antihypertensive agents have the potential to transfer into breast milk:
- consider monitoring the blood pressure of babies, especially those born preterm, who have symptoms of low blood pressure for the first few weeks
- when discharged home, advise women to monitor their babies for drowsiness, lethargy, pallor, cold peripheries or poor feeding. [2019]
1.9.4 Offer enalapril [5]to treat hypertension in women during the postnatal period, with appropriate monitoring of maternal renal function and maternal serum potassium. [2019]
1.9.5 For women of black African or Caribbean family origin with hypertension during the postnatal period, consider antihypertensive treatment with: nifedipine [3] or amlodipine if the woman has previously used this to successfully control her blood pressure. [2019]
1.9.6 For women with hypertension in the postnatal period, if blood pressure is not controlled with a single medicine, consider a combination of nifedipine [3] (or amlodipine) and enalapril [5]. If this combination is not tolerated or is ineffective, consider either: adding atenolol or labetalol to the combination treatment or swapping 1 of the medicines already being used for atenolol or labetalol. [2019]
1.9.7 When treating women with antihypertensive medication during the postnatal period, use medicines that are taken once daily when possible. [2019]
1.9.8 Where possible, avoid using diuretics or angiotensin receptor blockers [5] to treat hypertension in women in the postnatal period who are breastfeeding or expressing milk. [2010, amended 2019]
1.9.9 Treat women with hypertension in the postnatal period who are not breastfeeding and who are not planning to breastfeed in line with the NICE guideline on hypertension in adults. [2019]
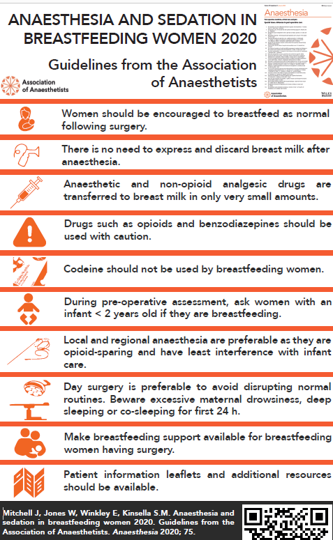
Anaesthesia and breastfeeding
I had the pleasure of working with a small team of anaesthetists for some time to develop guidelines so that breastfeeding mothers can have surgery, pain relief etc and continue to breastfeed as normal. The guideline also recommends support for the mother in terms of pumps, information and her baby nearby – not necessarily in that order.
In World Breastfeeding Week 2020 I was proud to share this guideline and infographic but sadly old habits seem to be coming back in with mothers advised incorrectly not to breastfeed for 24 hours after surgery. Policies seem to still need to be updated and training particularly of some pre-op nurses although many are up to date and well informed.
Guideline on anaesthesia and sedation in breastfeeding mothers is available in full at
https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/full/10.1111/anae.15179
Summary
Breastfeeding has many health benefits for the mother and infant. Women who are breastfeeding may require anaesthesia or sedation. Concerns regarding the passage of drugs into breast milk may lead to inconsistent advice from professionals. This can sometimes result in the interruption of feeding for 24 hours or longer after anaesthesia, or expressing and discarding (‘pumping and dumping’) breast milk; this may contribute to early cessation of breastfeeding. However, there are data regarding the transfer of most anaesthetic drugs into breast milk. We advise that breastfeeding is acceptable to continue after anaesthesia and should be supported as soon as the woman is alert and able to feed, without the need to discard breast milk. We provide evidence-based information on the pharmacokinetics of drugs commonly used during anaesthesia so that professionals can undertake a risk-benefit discussion with the woman. We advise the development of local policies that aid logistical planning and guide staff to facilitate breastfeeding during the woman’s hospital stay.
Recommendations
- Women should be encouraged to breastfeed as normal following surgery.
- There is no need to express and discard breast milk after anaesthesia.
- Anaesthetic and non-opioid analgesic drugs are transferred to breast milk in only very small amounts. For almost all drugs used peri-operatively, there is no evidence of effects on the breastfed infant.
- Drugs such as opioids and benzodiazepines should be used with caution, especially after multiple doses and in babies up to 6 weeks old (corrected for gestational age). In this situation, the infant should be observed for signs of abnormal drowsiness and respiratory depression, especially if the woman is also showing signs of sedation.
- Codeine should not be used by breastfeeding women following concerns of excessive sedation in some infants, related to differences in metabolism.
- Any women with an infant < 2 years should routinely be asked if they are breastfeeding during their pre-operative assessment.
- Opioid-sparing techniques are preferable for the breastfeeding woman. Local and regional anaesthesia have benefits in this regard, and also have the least interference with the woman’s ability to care for her infant.
- Where possible, day surgery is preferable to avoid disrupting normal routines. A woman having day surgery should have a responsible adult stay with her for the first 24 h. She should be cautious with co-sleeping, or sleeping while feeding the infant in a chair, as she may not be as responsive as normal.
- Breastfeeding support should be accessible for lactating women undergoing surgical and medical procedures.
- Patient information leaflets and additional resources should be available containing information on the compatibility of anaesthetic agents and analgesics during breastfeeding, and guidance on breastfeeding support in the peri-operative period.
Infographic guideline on anaesthesia and sedation in breastfeeding women
GP Presentation
Sharing a presentation which was given to GPs in the south west. Hopefully it is useful for professionals wanting to know more about prescribing for breastfeeding mothers
Monkeypox and breastfeeding
I sincerely hope this information is never needed but as of 6 june 2022 this is the recommendation on pregnancy and breastfeeding when a mother is suspected/proven to have monkeypox. This data is taken from the paper as below
RCOG 6 June 2022 New paper provides best practice for managing monkeypox in pregnancy (and breastfeeding) https://www.rcog.org.uk/news/new-paper-provides-best-practice-for-managing-monkeypox-in-pregnancy/
Highlights pasted from the paper below- basically we dont know about breastfeeding and the passage of monkeypox and need to protect the infant.
‘There is currently no evidence on the risk of viral transmission to the infant during breastfeeding, whether via the breast milk, direct contact with maternal skin lesions or via large droplet spread.
MVA-BN is considered safe in breastfeeding
Neonatal care
There is little evidence to guide neonatal care following the birth of a baby to a woman with monkeypox infection. Apart from macroscopic examination, the baby should undergo viral PCR testing either by throat swab or any lesions that are present. The baby should be isolated at birth from its mother and others, in a single room, with carers wearing appropriate PPE. The baby should be carefully monitored for signs of compromise or monkeypox infection. If the baby tests positive, the mother and baby can be reunited. Ideally, both mother and baby should be tested in parallel thereafter; after the mother is de-isolated (e.g. two negative PCR tests), mother and baby should be reunited. If a mother has reached a threshold to warrant PCR testing for the monkeypox virus, the baby should be isolated pending her swab result.
Breastfeeding
The proposed strategy for neonatal care would preclude most women with active monkeypox infection from breastfeeding their newborn. The WHO advises against breastfeeding; this seems reasonable in high-income country settings, such as the UK, in order to minimize the risk of neonatal monkeypox infection”
Proposed management of suspected or confirmed monkeypox infection in labor or if urgent delivery is needed.
• Advise delivery via Cesarean section
• Assess need for steroids and magnesium sulfate
• Maternity and neonatal staff to wear PPE
• Mother and baby should be isolated separately; avoid NNU admission if possible
• Mother should not breastfeed
• Encourage expressing so mother has opportunity to breastfeed after de-isolation; follow
recommendations for pump cleaning after each use
• Milk should be discarded as infected waste*
• Discuss with virologist testing needed
• If mother is negative, these precautions can be lifted
• If maternal infection confirmed, baby to be isolated for 3 weeks
• If both mother and baby test positive, they can be reunited https://obgyn.onlinelibrary.wiley.com/doi/pdf/10.1002/uog.24968

Monkeypox is usually a mild self-limiting illness, spread by very close contact with someone with monkeypox and most people recover within a few weeks. https://www.gov.uk/government/news/monkeypox-cases-confirmed-in-england-latest-updates
Symptoms
Initial symptoms of monkeypox include fever, headache, muscle aches, backache, swollen lymph nodes, chills and exhaustion. A rash can develop, often beginning on the face, then spreading to other parts of the body including the genitals. The rash changes and goes through different stages – it can look like chickenpox or syphilis, before finally forming a scab which later falls off.
Because the virus spreads through close contact, we are urging everyone to be aware of any unusual rashes or lesions and to contact a sexual health service if they have any symptoms.
“A notable proportion of recent cases in the UK and Europe have been found in gay and bisexual men so we are particularly encouraging these men to be alert to the symptoms” Dr Susan Hopkins, Chief Medical Adviser, UKHSA
UKHSA health protection teams are contacting people considered to be high-risk contacts of confirmed cases and are advising those who have been risk assessed and remain well to isolate at home for up to 21 days. In addition, UKHSA has purchased supplies of a safe smallpox vaccine (called Imvanex) and this is being offered to identified close contacts of someone diagnosed with monkeypox to reduce the risk of symptomatic infection and severe illness.
It’s very uncommon to get monkeypox from a person with the infection because it does not spread easily between people. But it can be spread through:
- touching clothing, bedding or towels used by someone with the monkeypox rash
- touching monkeypox skin blisters or scabs
- the coughs or sneezes of a person with the monkeypox rash
For full information from the UK Government and WHO see:
- The epidemiology, symptoms, diagnosis and management of monkeypox virus infections. https://www.gov.uk/guidance/monkeypox (May 2022)
The incubation period is the duration/time between contact with the infected person and the time that the first symptoms appear. The incubation period for monkeypox is between 5 and 21 days.
- World Health Organisation Monkeypox (May 2022) https://www.who.int/news-room/fact-sheets/detail/monkeypox
Transmission can occur via the placenta from mother to fetus (which can lead to congenital monkeypox) or during close contact during and after birth.
Vaccination with smallpox vaccine during breastfeeding
MVA-BN is not contraindicated if breast-feeding. It is not known whether MVA-BN is excreted in human milk, but this is unlikely as the vaccine virus does not replicate effectively in humans. Individuals who are breast feeding and have a significant exposure to monkeypox should therefore be offered vaccination, after discussion about the risks of monkeypox to themselves and to the breast-fed child. UKHSA Recommendations for the use of pre and post exposure vaccination during a monkeypox incident May 22 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1077678/Recommendations-for-use-of-pre-and-post-exposure-vaccination-during-a-monkeypox-incident.pdf?fbclid=IwAR2mS-bJgP3LLvvzNUS5aQf4SR3ZIdvg1Fn7XAxHTe7Vpm3KTDt0JPauNbg
Further information on monkeypox infection in pregnancy
- Kisalu NK, Mokili JL. Toward Understanding the Outcomes of Monkeypox Infection in Human Pregnancy. J Infect Dis. 2017;216(7):795-797. doi:10.1093/infdis/jix342 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6279131/?fbclid=IwAR1MVfVw9dQLR5ITTLEod3xhJAsvkdtLFkycDeIdIbBk-zja5CL4rlxNnFw
- Placide K Mbala, John W Huggins, Therese Riu-Rovira, Steve M Ahuka, Prime Mulembakani, Anne W Rimoin, James W Martin, Jean-Jacques T Muyembe, Maternal and Fetal Outcomes Among Pregnant Women With Human Monkeypox Infection in the Democratic Republic of Congo, The Journal of Infectious Diseases, 2017: 216 (7): 824–828, https://doi.org/10.1093/infdis/jix260 https://academic.oup.com/jid/article/216/7/824/4348689?fbclid=IwAR1MVfVw9dQLR5ITTLEod3xhJAsvkdtLFkycDeIdIbBk-zja5CL4rlxNnFw&login=false
Breastfeeding for Professionals – CPD
Back long ago before books and training material, let alone the website, I wrote a training pack for professionals with support from Roberta Roulstone from Peterborough Hospital. She inspired me to share my knowledge and changed my life. Another person who helped with the IT was Sarah Saunby a very great friend who I miss seeing.
This is an up to date version of that training which I have been picking up and putting down for a while. I hope it helps professionals to protect and support breastfeeding whilst adding to their own CPD.
For once I got round to recording it! But have included a link to the powerpoint as some links got covered up in my recording
Breastfeeding for Professionals Powerpoint
The substance exposed infant
This is an adapted version of a training powerpoint I gave some time ago. I plan to record it over the next few weeks and will upload it to my You Tube channel.
But hope it helpsin the meantime. Happy to answer any questions wendy@breastfeeding-and-medication.co.uk
Breastfeeding and the substance exposed infant
Providing effective, evidence based support for breastfeeding women in primary care
I was only involved in preparing one table of this article but it deserves to be widely shared as an excellent model of support for breastfeeding by all in primary care – doctors, nurses and pharmacists
BMJ article providing effective, evidence based support for breastfeeding women in primary care
Identifying the cause of breast and nipple pain during lactation
so proud and delighted to have worked with Lisa, Carmella and Jane over the past year to have this published in the BMJ today. To find out different practices across the world has been fascinating but I so hope this informs clinical practice
Identifying the cause of breast and nipple pain during lactation
Perinatal mental health and Breastfeeding
I have recorded the presentation which I have frequently given about perinatal mental health and breastfeeding. It should be used after listening to ” How drugs get into milk”
How do drugs get into breastmilk?
as it contains the pharmacokinetic data of drugs prescribed for perinatal mental health including SSRIs, anti anxiety medication and anti psychotics. It also includes research studies about the links between mental health and breastfeeding.
I hope this may increase prescriber’s knowledge as well as empower peer supporters and parents.