As with most professionals, my own included, dentistry seems to lack education on breastfeeding as part of undergraduate training if questions sent to this page exemplify a wider issue. I have tried to provide information for CPD inline with that written for other healthcare professionals.
I have developed this powerpoint presentation on the pharmacokinetics of drugs which dentists may use or prescribe for CPD information in an effort to break down the barriers of continuation of breastfeeding.
I am happy to answer individual questions or training. Please contact wendy@breastfeeding-and-medication.co.uk
In summary:
- Breastfeeding mothers can have local anaesthetic injections with/without adrenaline and continue to breastfeed as normal
- Breastfeeding mothers can take analgesics for dental pain and continue to breastfeed as normal
- Breastfeeding mothers can have antibiotics and continue to breastfeed as normal
- Breastfeeding mothers can use mouthwashes, gels and liquids for mouth ulcers ( e.g. Anbesol®, Bonjela®, Medijel®, Rinstead®, Iglu®, Orajel®) and fluoride toothpastes e.g. Durophat® and continue to breastfeed as normal
- Breastfeeding mothers can have dental sedation for procedures and continue to breastfeed as normal.
- White fillings: In some parts of the UK white fillings are recommended in pregnancy and lactation following an EU Directive (July 2018) but have to be paid for by the patient rather than being part of free NHS treatment. The information states that “These restrictions on the use of dental amalgam aim to help reduce environmental mercury pollution and are not a result of any safety concerns about amalgam fillings for dental patients.”
https://www.sdcep.org.uk/wp-content/uploads/2018/06/SDCEP-Dental-Amalgam-Information-for-Pregnant-or-Breastfeeding-Patients.pdf
- Tooth Whitening: There appears to be no information available on the use of tooth whitening agents during lactation. Whilst it is unlikely that any significant transfer of the agents used into breastmilk will take place, if it can be delayed until breastfeeding has finished naturally, that would be preferable but there are many questions from mothers about to get married who dont want to wait. Unless the products spill from the bath in which the liquid is placed, resulting in burns to the mother’s mouth absorption into breastmilk is unlikely.
For information on mercury fillings please see the information from InfantRisk December 2023
https://www.infantrisk.com/content/mercury-dental-fillings
Data suggests that maternal exposure to mercury vapor from dental amalgams or restoration is unlikely to have a significant impact on breastfeeding infants.
The established baseline for mercury levels in human breastmilk is set at ≥ 1 mcg/L.15 A comprehensive study examining mercury content in breast milk from mothers with dental amalgams revealed a range of mercury concentrations in human milk samples, spanning from < 0.2 to 6.86 mcg/L, with an average of 0.37 mcg/L.16 Studies have demonstrated transfer of mercury from a mother’s bloodstream to her breastmilk. Intriguingly, mercury levels in commercial formula samples displayed a broader spectrum, varying from 0.4 to 2.5 mcg/L on average, which was actually higher than the findings in the collected breastmilk samples.16
Remember, even if materials from mercury amalgams are orally ingested, elemental mercury is not absorbed from a healthy gastrointestinal tract. If a baby consumes miniscule mercury residues in breastmilk, it is likely that it wouldn’t be absorbed, especially as the baby ages and the GI tract matures.
Conclusion
Breastfeeding with mercury fillings or after dental amalgam restoration is likely safe and the benefits of breastfeeding outweigh the risks. Extra-cautious mothers could choose not to breastfeed for the first three days post-amalgam restoration, but the difference in infant risk will be miniscule.
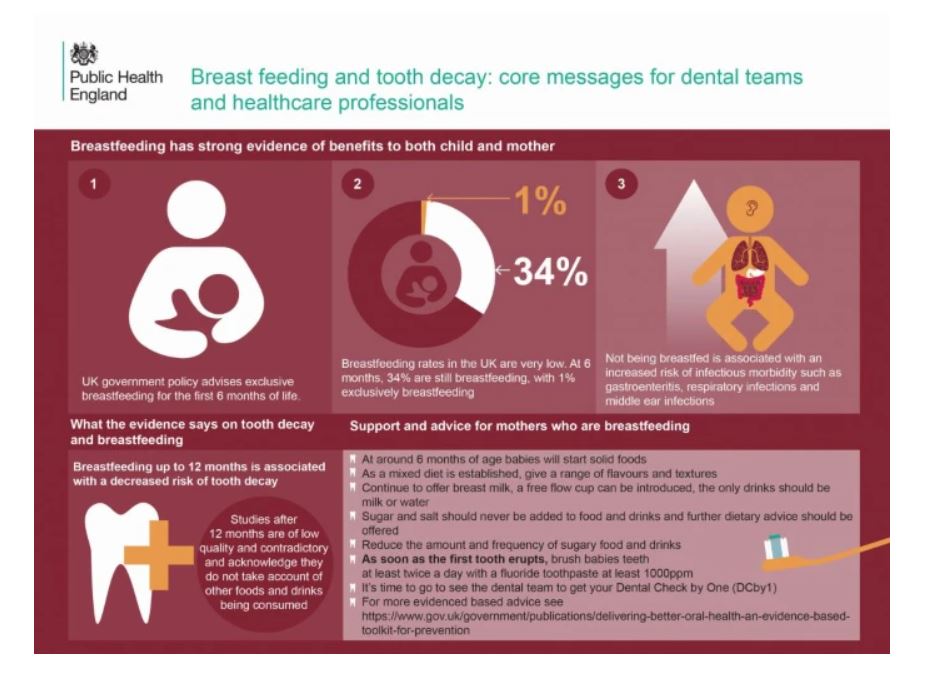
In a report Public Health England have made recommendations on dental health and breastfeeding. Full information can be accessed at : www.gov.uk/government/publications/breastfeeding-and-dental-health/breastfeeding-and-dental-health#breastfeeding-and-dental-health
- dental teams should continue to support and encourage mothers to breastfeed
- not being breastfed is associated with an increased risk of infectious morbidity (for example gastroenteritis, respiratory infections, middle-ear infections)
- breastfeeding up to 12 months of age is associated with a decreased risk of tooth decay
Delivering Better Oral Health (PHE, 2014 updated content 2017)4 recommends that:
- breast milk is the only food or drink babies need for around the first 6 months of their life, first formula milk is the only suitable alternative to breast milk
- bottle-fed babies should be introduced to drinking from a free-flow cup from the age of 6 months and bottle feeding should be discouraged from 12 months old
- only breast or formula milk or cooled, boiled water should be given in bottles
- only milk or water should be drunk between meals and adding sugar to foods or drinks should be avoided
Recent systematic reviews such as that by Tham and others (2015)6 included studies where children were breastfed beyond 12 months. When infants are no longer exclusively breast or formula fed, confounding factors, such as the consumption of potentially cariogenic drinks and foods and tooth brushing practices (with fluoride toothpaste), need to be taken into account when investigating the impact of infant feeding practices on caries development. Tham and others (2015) noted that several of the studies did not consider these factors and concluded that with regard to associations between breastfeeding over 12 months and dental caries “further research with careful control of pertinent confounding factors is needed to elucidate this issue and better inform infant feeding guidelines”. Good quality evidence on breastfeeding and oral health is an area with significant methodological challenges which have been outlined by Peres and others (2018)7.
Of course I would also have to highlight that dental procedures, including sedation, local and general anaesthetic and use of antibiotics and analgesics need not interrupt breastfeeding
Powerpoint training for dental practitioners on passage of drugs in breastmilk
See also: