Home » Articles posted by Wendy Jones (Page 2)
Author Archives: Wendy Jones
Betahistine and Breastfeeding
Betahistine (Serc ) is prescribed for dizzines and vestibular problems. There is little research available on it, because it isnt marketed in USA where most of the research studies are conducted. Anecdotally it is quite widely used without apparent problems. Observe the nursing baby for signs of drowsiness/ poor feeding in case
This is the entry I made for Breastfeeding and Medication 2018
“Betahistine is prescribed for vertigo, tinnitus and hearing loss associated with Ménière’s disease. There is no data on the amount that passes into breastmilk . It is an analogue of histamine and is believed to work by improving the microcirculationn of the labarynth. Side effects are reported to include gastro-intestinal disturbances, headache, pruritus and rashes. Prochlorperazine or cinnarazine would be the preferred to drug to treat dizziness. If betahistine use is perceived as essential the baby should be observed for drowsiness, GI disturbance and rash. There are no animal studies on use during lactation. Plasma levels of betahistine are very low. Plasma protein binding <5% (manufacturer SPC) Anecdotally it has been used without problems in breastfed babies “
See also https://www.e-lactancia.org/breastfeeding/betahistine/product/
Because of pharmacokinetic data it is likely excretion into breast milk, but though from very low plasma levels, usually below the detection threshold (100 pg/mL), so it is unlikely that the amount that could reach breast milk is significant.

Agnus Castus and Breastfeeding
I am not going to pretend that I am an expert on complimentary medicine but I am frequently asked about Agnus Castus for fertility and menstrual issues so am including this information based on the LactMed entry
Agnus Castus and Breastfeeding Fact Sheet
Other information may be found in :
- Herbs and Breastfeeding: References. https://kellymom.com/bf/can-ibreastfeed/herbs/herbal-ref/
- Herbal safety for nursing moms. https://kellymom.com/bf/can-ibreastfeed/herbs/herbal_safety/
- The Nursing Mother’s Herbal 2003 by Shelia Humphrey. Available from Amazon £9.99
Agnus-castus (Chasteberry) is from the berries of the chaste tree. The berries contain essential oils Chasteberry is often used for irregularities of the menstrual cycle, infertility, premenstrual complaints, and cyclical breast pain. [Dennehy 2006]
In low doses, chasteberry increases serum prolactin and it is a purported to increase milk supply (a galactogogue). [Javan 2017] however, no scientifically valid clinical trials support this use. Galactogogues should never replace evaluation and counselling on modifiable factors that affect milk production. [ Brodribb 2017, ACOG 2021] Some evidence indicates that high doses of chasteberry decrease serum prolactin and might decrease lactation. [ Eglash 2014 ] It has been used to decrease breastmilk oversupply in Persian traditional medicine.[Kabiri 2017]
In general, chasteberry is well tolerated. The most frequent adverse events are nausea, headache, gastrointestinal disturbances, menstrual disorders, acne, pruritus, and erythematous rash; however, all are mild and reversible. Among 352 nursing mothers given chasteberry tincture, 15 cases of pruritus, exanthema, urticaria, and some cases of early menstrual period occurred. Because of concerning safety data and possible lactation suppression, chasteberry should be avoided during lactation. [Daniele 2005]
See also https://www.e-lactancia.org/breastfeeding/vitex-agnus-castus/writing/
References
- Dennehy CE. The use of herbs and dietary supplements in gynaecology: an evidence-based review. J Midwifery Womens Health. 2006; 51:402–9. https://pubmed.ncbi.nlm.nih.gov/17081929/
- Javan R, Javadi B, Feyzabadi Z. Breastfeeding: A review of its physiology and galactogogue plants in view of traditional Persian medicine. Breastfeed Med. 2017; 12:401–9. https://pubmed.ncbi.nlm.nih.gov/28714737/
- Brodribb W. ABM Clinical Protocol #9. Use of galactogogues in initiating or augmenting maternal milk production, second revision 2018. Breastfeed Med. 2018; 13:307–14. https://pubmed.ncbi.nlm.nih.gov/29902083/
- Breastfeeding challenges: ACOG Committee Opinion, Number 820. Obstet Gynecol. 2021;137: e42–e53. https://pubmed.ncbi.nlm.nih.gov/33481531/
- Eglash A. Treatment of maternal hypergalactia. Breastfeed Med. 2014; 9:423–5 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4216483/
- Kabiri M, Kamalinejad M, Sohrabvand F, et al. Management of breast milk oversupply in traditional Persian medicine. J Evid Based Complementary Altern Med. 2017; 22:1044–50 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5871304/
- Daniele C, Thompson Coon J, Pittler MH, et al. Vitex agnus castus: A systematic review of adverse events. Drug Saf. 2005; 28:319–32. https://pubmed.ncbi.nlm.nih.gov/15783241/
Pain relief after a c section and Breastfeeding
This week I posted a link to a recently published paper which concluded that poor pain relief after a C section affected breastfeeding. https://consultqd.clevelandclinic.org/following-cesarean-delivery-postoperative-pain-affects-likelihood-of-in-hospital-breastfeeding/
I was saddened that we even had to think that pain would not be managed well for any mother, let alone when she was trying to initiate breastfeeding. It isn’t always easy to life a baby from a cot side crib when you have had surgery, let alone try to position a baby to achieve the perfect latch.
What surprised and horrified me was the mother’s who replied that they hadnt been given good pain relief when in hospital. They mentioned:
- not being told that more than paracetamol was available
- being offered only paracetamol and ibuprofen even when they needed more
- being forgotten on medication rounds,
- being discharged without sufficient pain relief.
This just isnt good enough and I would hope that everyone to whom this applies contacts the ward directly or through PALS that pain management plans are essential.
Pain relief which should be given to a breastfeeding mum in my opinion:
- In theatre a non steroidal anti inflammatory eg diclofenac as a suppository
- On the ward there should be available oramorph (subject to extensive first pass metabolism so little in milk)
- Regular use of an NSAID – ibuprofen, diclofenac or naproxen (low levels in milk) plus paracetamol See https://www.sps.nhs.uk/articles/using-nsaids-during-breastfeeding
- Codeine is no longer recommended but dihydrocodeine can be offered https://breastfeeding-and-medication.co.uk/thoughts/breastfeeding-and-codeine
- (https://breastfeeding-and-medication.co.uk/thoughts/dihydrocodeine-and-breastfeeding)
- Discharge packs should include the NSAID offered in hospital plus limited number of dihydrocodeine(usually 5 days supply) and if necessary although rarely oramorph. This may challenge the formulary in the hospital but can be overcome simply with care and thought for the patient.
- All opioids can cause nausea and dizziness but almost invariably cause constipation so it is wise to commence stool softeners like lactulose and/or docusate both of which are compatible with breastfeeding as they don’t pass into milk.
- Breast milk oxycodone concentrations in mothers given oxycodone for post-Caesarean delivery pain management. https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/bcp.16008
NO WOMAN SHOULD BE LEFT IN PAIN BECAUSE SHE IS BREASTFEEDING
Breastfeeding after CT and MRI scans
Virtually every day I get messages from mothers and health visitors querying whether mothers can continue to breastfeed after CT and MRI scans. I was told that the national guidelines had been updated some years ago to align with RANZR guidelines . Sadly guidelines dont seem to have been updated by all radiology departments from my experience despite an update on 25.1.22 (see below)
I was lucky enough to work with Dr Gabrielle Cronin on this paper which was published in the Irish BMJ
Most mothers are advised to stop breastfeeding for 24 hours but there is no evidence for this as most contrast media are not orally bio available and have half lives which do not justify this duration.
On 25 January 2022 this was published by the Society of Radiologists :
https://www.sor.org/news/sor/sor-issues-joint-statement
The Society has issued guidance to reassure patients after recent research showed a lack of awareness among imaging teams on the most up-to-date evidence and guidance for breast-feeding patients who require a CT or MRI with contrast.The current Royal College of Radiologists (RCR) guidance published in 2019 relating to MR states:While no special precaution or cessation of breastfeeding is required the continuation or cessation of breastfeeding for 24 hours should be at the discretion of the lactating mother in consultation with the clinician.The SoR and RCR refer to the guidance published by The Royal Australian and New Zealand College of Radiologists (RANZCR) regarding CT contrast which says:Cessation of breast feeding or expression and discarding of breast milk after iodinated contrast media administration are not required.The Breastfeeding Network has summarised the advice of a number of expert organisations across the globe which is available on their website .The very small potential risk associated with absorption of contrast medium is considered insufficient to warrant suspending breastfeeding for any period following iodinated contrast agent administration.It is the view of the RCR and SoR that patients who wish to continue breastfeeding after being administered with contrast agent should be able to do so as there is no evidence of risk to the baby/child.Position statement – for patients. The Society of Radiographers (SoR) and the Royal College of Radiologists (RCR) are aware of conflicting opinions about whether patients who are administered with contrast agents – usually as part of a CT or MRI scan– can breast feed as part of their normal routine.It is the view of both the RCR and the SoR that patients who wish to continue breastfeeding after being administered with contrast agent – usually given in advance of a CT or MRI scan – should be able to do so as there is no evidence of risk to the baby/child. If you have any concerns please, speak with your radiographer or radiologist.
More information
https://www.breastfeedingnetwork.org.uk/ct/ https://www.breastfeedingnetwork.org.uk/mri/
Ulipristal Acetate (EllaOne) as an emergency hormonal contraceptive and Breastfeeding
Ulipristal is used as an emergency contraceptive for up to 120 hours (5 days) after intercourse. It is a single tablet.
The manufacturer (patient information leaflet and SPC) recommends that breastfeeding should be avoided for 1 week after administration as it is present in milk.
This does not seem to be justified by pharmacokinetic data which supports the recommendations by expert sources that breastfeeding can continue as normal.
The specialist pharmacy service (October 2023) recommended that along with other hormonal method of emergency contraception it is compatible with breastfeeding if other methods are not appropriate ” Very limited evidence shows it is excreted in negligible levels into breast milk. It is highly bound to plasma proteins which limits its excretion into breast milk. Despite its long half-life, the single dose for emergency contraception is unlikely to result in accumulation in infants. Although, there is no information on infant serum levels, based on milk levels reported and the properties of ulipristal acetate, infant levels are predicted to be low and infant side effects would not be expected. No interruption of breastfeeding is considered necessary after taking a single dose. https://www.sps.nhs.uk/articles/using-emergency-contraception-during-breastfeeding
Pharmacokinetics
It is highly plasma protein bound (98-99.5%)
Relative Dose 0.8 – 1 % (significantly below 10% regarded as compatible with breastfeeding)
The manufacturer reports that after this medication was given to 12 breastfeeding women for emergency contraception mean levels in milk were measured as shown
| ulipristal level in breastmilk | |
| 24 hours | 22.7 ng/mL |
| 24-48 hours | 2.6ng/ml |
| 48-72 hours | 1.56 ng/mL |
| 72-96 hours | 1.04 ng/mL |
| 96-120 hours | 0.69 ng/mL |
The manufacturer did not report any neonatal outcomes as the infants in this report were not breastfed.
Recommendations on compatibility of breastfeeding
- No information is available on the clinical use of ulipristal during breastfeeding; however, amounts in milk are low. If ulipristal is required by the mother, it is not a reason to discontinue breastfeeding. Some older sources recommend withholding breastfeeding for 24 hours after a dose,[ Curtis KM, Jatlaoui TC, Tepper NK, et al. U.S. selected practice recommendations for contraceptive use, 2016. MMWR Recomm Rep. 2016;65:1–66]but this is no longer a requirement according to current FDA-approved labeling. https://www.ncbi.nlm.nih.gov/books/NBK500655/
- Intestinal absorption by the infant of the low dose excreted in breastmilk would be hindered, since oral bioavailability decreases up to 45% if administered with fat-rich foods, such as breastmilk.
Given the minimal excretion of the product in breastmilk and the absence of adverse effects recorded during breastfeeding, it is difficult to justify the recommendation proposed by other authors or health agencies such as CDC to interrupt breastfeeding for 24 hours (Curtis 2016 CDC) or 36 hours (Mansour 2009).
https://www.e-lactancia.org/breastfeeding/ulipristal-acetate-contraceptive/product/
- A single dose of 30mg ulipristal acetate is licensed to be taken within 120 hours (5 days) after unprotected intercourse or contraceptive failure. Ulipristal is not the preferred emergency contraceptive during breastfeeding, however, based on pharmacokinetic data, UKDILAS do not consider it necessary to withhold breastfeeding if a single dose has been taken. https://www.sps.nhs.uk/articles/emergency-contraception-and-breast-feeding/
Patient advice
- if vomiting occurs within 3 hours of taking a dose, a replacement dose should be taken;
- the next period may be early or late;
- seek medical attention promptly if any lower abdominal pain occurs because this could signify an ectopic pregnancy.
- Take a pregnancy test if the next menstrual period is delayed by more than 7 days, is lighter than usual, or is associated with abdominal pain which is not normal for a period pain
Further sources of information
Anti epilepsy medication and breastfeeding
A brief introduction to the information on the safety of anti epilepsy medication during breastfeeding. It does not include full information but you can find more in my book or by emailing me.
pdf of this factsheet available:
It is difficult to provide all the information on anti-epileptic medication in a fact sheet. If you need more information you might like to buy my book (Breastfeeding and Medication 2018)! Or you can email me (wendy@breastfeeding-and-medication.co.uk). The information below is taken briefly from text in my book.
It is absolutely imperative that you do not stop taking your medication in order to breastfeed. Your baby needs you to be seizure free. I cannot imagine the risk to your baby in the home if you are alone, maybe at a bus stop or back driving having been well controlled.
Many of the drugs can be taken by breastfeeding mothers. There will be a caution to observe the baby for drowsiness and poor feeding with each one. If you take more than one drug that risk would increase. This doesn’t mean you can’t breastfeed just that we need to keep that information in our minds and ensure that the baby is feeding and growing. If he/she isn’t growing we may need to consider options and support.
Many mothers ask if they can time breastfeeds so that the baby gets a minimal level of drug. Once you have taken any drug for more than 3 days it reaches a steady state with little fluctuation across the 24-hour period. This is essential as we don’t want a time of the day when your medication falls below an effective level. So, there are no peaks and troughs in which to feed or avoid feeding.
Some mothers know that their seizures may be precipitated by tiredness so they need to find ways of getting as much rest as possible. This might be using some formula or another adult bringing the baby to you to feed then caring for it. If you are very tired be very careful with co-sleeping as you may lose your natural awareness of the baby ( www.basisonline.org.uk has more information)
Different people require different medication to stabilise epilepsy. This fact sheet is one I have tried to write several times. There is so much to discuss with individual mothers, this can only be an introduction. Please message me if you need more information or to discuss the facts presented very briefly here.
Anti-epilepsy medication
- Lamotrigine (Lamictal ®): watch baby for drowsiness and any strange rash. If your dose
was increased in pregnancy you will need a blood test soon after birth and will probably
have your dose reduced. Lamotrigine is present in milk, but limited data suggests no harmful
effect on the infant. - Topirimate (Topamax®):Öhman et al 2002. observed five babies at delivery and followed
three of them through lactation. Two to three weeks after delivery two of the breastfed
infants had detectable but unquantifiable levels of topiramate and one had an undetectable
concentration; m/p ratios of around 0.86 were determined throughout the study period and
no adverse events noted. Observe for sedation, poor feeding and diarrhoea. - Levetiracetam(Keppra ®): Johannessen et al. (2005) studied eight women with maternal
doses of levetiracetam up to 3.5 g daily, which produced low levels in milk and no adverse effects in their breastfed infants. The babies of mothers taking levetiracetam should be monitored for drowsiness and adequate weight gain. - Vigabatrin (Sabril ®): This drug is used where control of seizures has not been achieved.
Tran et al. (1998) studied two mother and baby pairs. He estimated the maximum amount of vigabatrin that a suckling infant would ingest in a day is 3.6% and 1% of the weight-adjusted daily dose respectively. It irreversibly inactivates gamma-aminobutyric acid (GABA) and the effect of this on neonatal brains is unknown. However, it is used directly to control infant spasms. Observe for sedation - Carbamazepine (Tegretol ®): It reaches measurably detectable levels in infant serum but
below the therapeutic range. The infant should be monitored for jaundice, drowsiness and adequate weight gain as sedation, poor sucking and hepatic dysfunction have been
reported, although rarely. - Sodium valproate (Epilim): this drug is now more rarely seen due to its known
teratogenic effects (MHRA 2017). Low levels are found in breastmilk but theoretically it is
recommended that the baby should be monitored for jaundice and liver damage. - Phenytoin (Epanutin®): All studies of phenytoin show levels in breastmilk to be too low to cause difficulties for breastfed infants
References - Jones W Breastfeeding and Medication 2nd Ed 2018 . Routledge
- Veiby G, Engelsen BA, Gilhus NE, Early child development and exposure to antiepileptic
drugs prenatally and through breastfeeding:a prospective cohort study on children of
women with epilepsy, JAMA Neurol, 2013Nov;70(11):E1–E8. - Ohman I, Vitols S, Luef G, Söderfeldt B, Tomson T, Topiramate kinetics during delivery,
lactation, and in the neonate: preliminary observations, Epilepsia, 2002;43:1157–60. - Johannessen SI, Helde G, Brodtkorb E, Levetiracetam concentrations in serum and in
breastmilk at birth and during lactation, Epilepsia, 2005;46:775–7 - Tran A, O’Mahoney T, Rey E, Mai J, Mumford JP, Olive G, Vigabatrin: placental transfer in
vivo and excretion into breastmilk of the enantiomers, Br J Clin Pharmacol, 1998;45:409–11 - MHRA, Valproate and Developmental Disorders: New Alert Asking for Patient Review and
Further Consideration of Risk Minimisation Measures, MHRA, 2017, www.gov.uk/drugsafety-update/valproate-and-developmental-disorders-new-alert-asking-for-patient-reviewand-further-consideration-of-risk-minimisation-measures.
Antibiotics and Breastfeeding
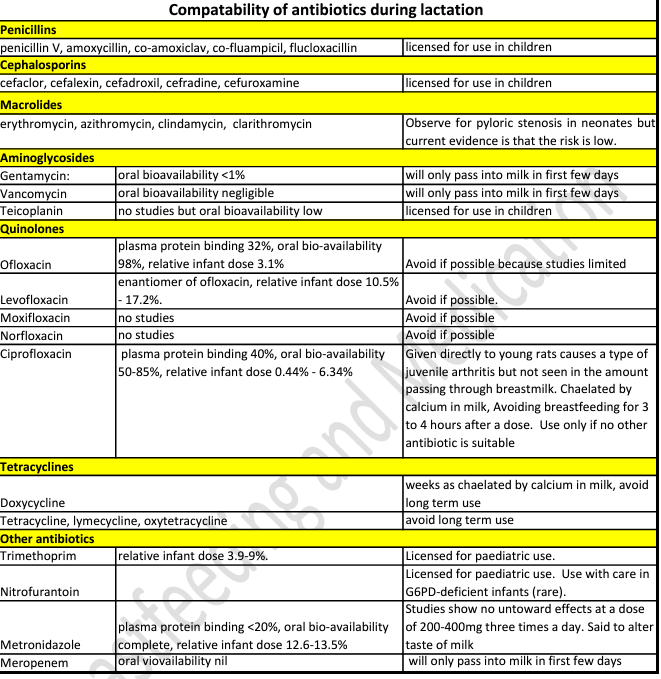
Although we now try very hard to avoid prescribing antibiotics unless essential ( because of the risk that in the future we wont have antibiotics which are as effective against all infections), sometimes they are necessary. The use of antibiotics during breastfeeding often causes disquiet because most of them cause the baby to have loose bowel motions, sometimes tummy cramps, and sometimes vomiting. Is continuing to breastfeed actually causing harm and should feeding be interrupted? Do we need pre-biotics and probiotics to redress the balance in the baby’s gut?
It is hard to watch a baby in distress but it is important to remember that when we breastfeed during an infection we are also passing antibodies to that infection in breastmilk to protect the baby. Breastmilk contains all the factors to redress the balance and return the baby’s gut to its normal state far better than any probiotics derived from other sources, in my opinion.
But the ultimate choice is that of the breastfeeding mother.
January 2024 the MHRA issued guidance on fluoroquinolones : ” that fluoroquinolone antibiotics given systemically (by mouth, injection, or inhalation) must only be administered when no other antibiotics are appropriate for use, the Medicines and Healthcare products Regulatory Agency (MHRA) has announced. This means that fluoroquinolones should only be prescribed when other recommended antibiotics have failed, will not work due to resistance, or are unsafe to use in an individual patient.” https://www.gov.uk/government/news/mhra-introduces-new-restrictions-for-fluoroquinolone-antibiotics
Fluoroquinolone include ciprofloxacin, levofloxacin, moxifloxacin, and ofloxacin. If prescribed these as a first option please discuss with your prescriber. The MHRA guidance refers to use in adults only where no other antibiotic is available.
See also https://www.sps.nhs.uk/articles/using-metronidazole-during-breastfeeding
Metronidazole can be used during breastfeeding for most usual treatment courses. Recommendations apply to full term, healthy infants.
I hope that the information in this factsheet helps make that decision. Please email me if you want to discuss anything : wendy@breastfeeding-and-medication.co.uk
Antibiotics and breastfeeding factsheet pdf
Antibiotics are acknowledged to be overused which is one of the reasons that Multiple Resistant Staphylococcus aureus (MRSA) and Clostridium difficile have become more widespread. It is sensible to consider whether a mother needs to be treated with antibiotics before exposing both her and her breastfed baby. Babies exposed to antibiotics via their mother’s breastmilk may develop symptoms of colic, abdominal discomfort and diarrhoea. These are an inconvenience and not a reason to suspend breastfeeding. Research undertaken in Canada in 1993 (Ito et al. 1993) showed that 15% of women prescribed antibiotics chose not to take the medicine and continue to breastfeed, rather than expose their baby to a risk which they had been assured was minimal. By contrast, 7% stopped breastfeeding during therapy despite reassurance. The research team also examined the reporting of adverse effects by mothers made aware of potential diarrhoea in the child with antibiotics passing through breastmilk. Although more women warned of side effects reported clinical effects which they had noted and judged to be due to the medication, than those not made aware, the difference is not statistically significant (87% compared with 68%). No difference in compliance with the antibiotic regimen or breastfeeding pattern, were noted between the two groups (Taddio et al. 1995).
These follow recommendations from the doctor that the ‘infection’ may be self-limiting but if symptoms develop further or fail to resolve in the following 48 hours, then the course of antibiotics should be taken. Little et al. have suggested restricting the use in the treatment of otitis media, upper respiratory infection and sore throat ((Little 2002; 2005; 1997) beginning the public health message about reducing the use of antibiotics. It may also be useful in the management of mastitis.
References
• Abdellatif M e, Ghozy S, Kamel MG, Elawady SS Ghorab MMEAttia AW, Le Huyen TT, Duy DTVHirayama K, Huy NT. Association between exposure to macrolides and the development of infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis. Eur J Pediatr. 2019 178(3):301-314.
• Hale T. Hale’s medications & mothers’ milk. 19th ed. New York, USA: : Springer Publishing 2021. • Ito S, Koren G, Einarson TR, Maternal non compliance with antibiotics during breastfeeding, Ann Pharmacother, 1993;27(1):40–42.
• Ito S, Koren G, Einarson TR. Maternal Noncompliance with Antibiotics during Breastfeeding. Ann Pharmacother 1993;27:40–2. doi:10.1177/106002809302700110 • Jones W Breastfeeding and Medication Routledge 2018
• Jones W How to advise women on the safe use of medicines while breastfeeding The Pharmaceutical Journal, PJ, 2021, 306 (7949) https://pharmaceuticaljournal.com/article/ld/how-to-advise-women-on-the-safe-use-of-medicines-whilebreastfeeding
• LactMed https://www.ncbi.nlm.nih.gov/books/NBK501922/ • Little P, Delayed prescribing of antibiotics for upper respiratory tract infection, BMJ, 2005;331(7512):301.
• Little P, Gould C, Moore M, Warner G, Dunleavey J, Williamson I, Predictors of poor outcome and benefits from antibiotics in children with acute otitis media: pragmatic randomised trial, BMJ, 2002;325(7354):22
• Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth AL, Open randomised trial of prescribing strategies in managing sore throat, BMJ, 1997;314:722.
• Taddio A, Ito S, Einarson TR, Leeder JS, Koren G, Effect of counselling on maternal reporting of adverse effects in nursing infants exposed to antibiotics through breastmilk, Reprod
See also https://www.sps.nhs.uk/articles/using-tetracycline-antibiotics-during-breastfeeding
https://www.sps.nhs.uk/articles/using-macrolide-antibiotics-during-breastfeeding
https://www.sps.nhs.uk/articles/treating-impetigo-topically-during-breastfeeding
Nausea and Breastfeeding
One of the more frequently asked questions recently relates to nausea and even vomiting when breastfeeding. It may be due to norovirus, pregnancy (see https://breastfeeding-and-medication.co.uk/fact-sheet/vomiting-in-pregnancy-whilst-still-breastfeeding ) or to stop nausea from medication e.g morphine.
I hope this factsheet provides some options. The information is taken from my book Breastfeeding and Medication which provides more details and references. Maybe you need to buy a copy?
Nausea can be triggered by a variety of factors including food poisoning, motion sickness, labarynthitis, vertigo, pregnancy, migraine or as a symptom of other underlying conditions.
Cinnarazine (Stugeron®)
Cinnarazine is used for symptomatic treatment of nausea and vertigo caused by Ménière’s disease as well as prevention of travel sickness. There are no data on transfer into breastmilk but it is licensed for use in children.
Probably compatible with use during breastfeeding. Although there are no data on transfer into breastmilk, it is licensed for use in children.
Prochlorperazine ( Stemetil®, Buccastem®)
Prochlorperazine is used to treat vertigo, labarynthitis, migraine or drug-induced emesis. Its oral bio-availability is low due to high first-pass metabolism. Long-term use should be avoided in breastfeeding where possible, particularly with very young babies where there is a potential risk of apnoea. However short-term acute use probably poses few risks as it is licensed for use in children over 10 kg.
Compatible with use during breastfeeding if used short term. Avoid long term or where child is at risk of apnoea.
Domperidone (Motilium®)
Domperidone stimulates gastric emptying. It causes fewer central effects such as sedation and dystonia (although there are still reports of these) because it does not cross the blood–brain barrier. Its dopamine antagonist activity stimulates prolactin release, which makes it useful as a galactagogue.
Domperidone is metabolised by cytochrome P450 so care should be taken with potential interactions. It is more than 90% bound to plasma proteins and has a low bio-availability on an empty stomach (15%) when taking orally due to first-pass hepatic and intestinal metabolism.
Doses of more than 60 mg per day have been associated with sudden cardiac death although reports have been predominantly in the elderly and in those receiving intravenous doses (FDA 2004, Joss et al. 1982, Giaccone et al. 1984, Weaving 1984, Roussak 1984, Osborne et al. 1985, manufacturers information 2012).
Compatible with use during breastfeeding due to extensive plasma protein binding. See also information as a galactogogues.
Metoclopramide (Maxolon®, Migravess®, Paramax®)
Metoclopramide is a dopamine antagonist and can cause extra-pyramidal side effects, in particular, acute dystonia. This adverse effect is most commonly seen in children and young adults, especially females, so it is not a drug of choice in lactating mothers who generally fall into this age group. It may also precipitate hypotension and depression. Other side effects reported include headache, diarrhoea, dry mouth and change in appetite (Ingram et al. 2011). It stimulates prolactin secretion and has been used as a galactogogue but has now been superseded. The bio-availability of oral metoclopramide is about 75% but varies widely between patients due to its hepatic first-pass metabolism. Concentrations higher than those in maternal plasma may be reached in breastmilk particularly in the early puerperium, although these decrease with increased maturity.
Compatible with use during breastfeeding but avoid if possible due to risk of extrapyramidal effects and link with depression. Use domperidone as an alternative.
Cyclizine (Valoid®)
Cyclizine is an anti-emetic used to treat motion sickness, post-operative nausea and vomiting, after radiotherapy, and in drug- induced situations as well as nausea in pregnancy. There are no reports of levels entering breastmilk (BNF) or data on which to base conclusions. There is an unlicensed dose for children aged over 6 years.
Avoid if possible as no information on passage into breastmilk although if use considered essential unlikely to produce adverse effects if used short term. Longterm use may cause drowsiness in baby and consequent weight loss.
Hyoscine (Joy Rides®, Kwells®)
Hyoscine produces a reduction in salivation as well as some sedation. It is commonly used to prevent travel sickness as well as other types of nausea, either as an oral tablet or as a patch. It is believed to pass into breastmilk but no studies report the amounts. No reports of adverse effects appear to have been made and it appears compatible with breastfeeding, particularly to prevent travel sickness. Long-term use could decrease lactation.
BNF suggests that the amount in breastmilk is too small to be harmful.
Safe to use during breastfeeding to prevent travel sickness. No studies on passage into breastmilk but no adverse events reported so safety presumed as used in paediatric doses.
Ondansetron ( Zofran®)
This drug is a 5-HT3 antagonist with antiemetic activity. It is used in the management of nausea and vomiting induced by cytotoxic chemotherapy and radiotherapy. It is also used for the prevention and treatment of post-operative nausea and vomiting that have not responded to other antiemetic agents. Ondansetron may also be used for nausea in pregnancy. It is licensed for use in children from two years of age. It is 60% orally bio-available and 70–75% plasma protein bound. The terminal half-life is 3 hours after oral doses. There are no studies on transfer into breastmilk although it has been found in animal studies (BNF).
Avoid if possible as no information on passage into breastmilk but licensed for use in children > 2 years.
See also https://www.sps.nhs.uk/articles/treating-nausea-during-breastfeeding
Hypertension (raised blood pressure) and Breastfeeding
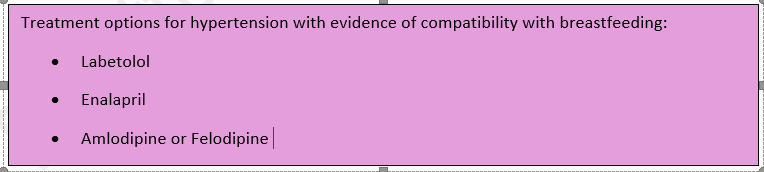
Many mothers experience raised blood pressure it seems. Is this due to our busy lifestyles, more mums giving birth at an older age? Who knows but it causes a lot of confusion. The drug normally initiated if a mother has symptoms of pre-eclampsia is labetolol. It is usually continued after delivery until the BP has settled. Virtually none passes into breastmilk. However, some mothers with poor circulation may notice sore, white nipples where the supply to the tip is decreased . If this happens the drug may need to be changed. Prolonged high BP in pregnancy can lead to restricted growth of the baby who may be born sleepy. Rather than just monitoring blood glucose levels the baby should be helped to attach to the breast and feed regularly or be given colostrum by spoon or syringe. A drop of colostrum can work magic.
Later blood pressure rises can be treated with enalapril, amlodipine and felodipine which are all compatible with breastfeeding according to expert sources. The NICE Guidelines NG 133 (2019) can also guide good practice.
The data for this fact sheet is taken from my book Breastfeeding and Medication which provides more detail and references to studies. Please consider buying a copy for future reference.
There is much information in this factsheet.
Hypertension (raised blood pressure) is defined as sustained blood pressure above 140/90. Diet, obesity, heredity, race and stress all impact on blood pressure. High cholesterol, high salt content in the diet and saturated fat intake increases the long-term health risk.
Breastfeeding women may have had a previous event which presents a challenge to pregnancy and lactation e.g., stroke, heart attack, renal complications, SVT etc. In the past these might have produced barriers to childbirth but now seem to be so well controlled mothers are able to give birth and look after their own health.
There are several types of drugs used to treat hypertension some of which we have no data on with respect to use in breastfeeding mother, others should be avoided where possible.
For more details and references see Breastfeeding and Medication Jones W Routledge 2018
Diuretics
All diuretics should be avoided unless essential for health of the mother. By removing excess fluid from the body diuretics may reduce milk supply. This is more likely with furosemide than Bendroflumethiazide or bumetanide, but this category of drugs should be avoided during lactation to control blood pressure but only fluid retention, where essential
Bendroflumethiazide – unknown effect from low dose 2.5mg daily
Indapamide – No information is available on the amount of indapamide in breastmilk. Intense diuresis with large doses may decrease breastmilk production.
Furosemide – more likely to reduce supply due to intense diuresis
Bumetanide – low risk in established supply
Spironolactone – an aldosterone receptor antagonist used as a diuretic in various conditions associated with oedema, as well as in the treatment of hypertension. Its value is in sparing potassium loss. It is metabolised to canrenone which was found in the breastmilk of one mother taking 25mg four times a day by Phelps (1977). He suggested the amount absorbed by the baby would be 0.2% of the mother’s daily dose. Spironolactone is 90% plasma protein bound and has a bioavailability of 90% (Martindale 2017) 70% (Hale 2017). The American Academy of Paediatrics considers it compatible with breastfeeding. The BNF states that although its metabolite is present in milk, the amount is probably too small to be harmful.
ACE inhibitors
This family of drugs are potentially teratogenic but can be used during lactation
Enalapril. This is the ACE with most evidence of safety during lactation. Redman et al. (1990) studied five women taking 20 mg enalapril, it was not detectable after 4 hours in four of the five women while the average peak level of enalaprilat (the metabolite of enalapril) was 1.7 µg per litre. No adverse events were reported in four babies exposed to maternal levels of 5–10 mg. Huttenen et al. (1989) studied three women after single doses of enalapril up to 10 mg. Enalaprilat levels were not detected and the concentration of ACE activity in milk was unchanged. Rush et al. (1989) deduced that the total amount of enalapril and its metabolite to which a baby would be exposed was 2 µg of enalaprat while unlicensed use of enalapril from 1 month (BNFC) is 100 µg per kilogramme per day. Relative infant dose quoted as 0.2% (Hale 2017 online access).
BNF data recommend that the drug is avoided in the first few weeks after delivery due to the risk of profound neonatal hypotension; it can be used in older infants if essential but recommends that the infant’s blood pressure is monitored.
Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Captopril: Devlin and Fleiss’ study (1981) of 12 women showed that the concentration of captopril in breastmilk was about 1% of maternal plasma, equivalent to 4.7 µg per litre in breastmilk of mothers taking 300 mg daily and no adverse effects were noted in the babies. Compatible with breastfeeding. Amount transferred into breastmilk is significantly less than can be given directly to a baby more than 1 month of age.
Ramipril: No data are available on transfer into breastmilk. Ramipril has an active metabolite ramiprilat, which is approximately 56% plasma protein bound.
Lisinopril: There is no information on the transfer of lisinopril into breastmilk, although the oral bioavailability is only 29%. It is not significantly bound to plasma proteins.
Perindopril: There are no data available on the transfer of perindopril into breastmilk. It is metabolised to perindoprilat which is the active drug. Plasma protein binding is reported to be 10–20% and oral bioavailability is 65–75%.
Quinapril: rapidly converted to its active metabolite quinaprilat. Begg studied 6 women taking 20mg quinapril daily. Four hours after the dose no drug was recovered from milk. No Quinaprilat was detected at any time. The authors therefor suggested that quinapril is safe in breastfeeding.
Beta blockers
Beta blocker of choice in a mother during breastfeeding based on evidence of benefit and safety for the baby is Metoprolol, propranolol or labetolol
In many maternity units the use of beta blockers triggers the hypoglycaemia policy involving blood sugar testing. The amount of labetolol, propranolol and metoprolol passing into breastmilk is low and these drugs are less likely to lower blood sugars than atenolol (which has low plasma protein binding and passes more extensively into milk). The risk to the baby stems from the fact that babies born to mothers with pre-eclampsia may be born (or induced) early or may have experienced intra-uterine growth retardation. The efficacy of the baby’s feeding and milk transfer should be assessed as well as blood sugars. If necessary, the mother may need to hand express and syringe/cup/spoon feed colostrum to her infant.
Atenolol: diffuses into breastmilk in concentrations similar to or higher than those in maternal blood demonstrated by m/p ratios of 1.5–6.8. Despite this, the authors calculated the infant would only be exposed to 0.13 mg per day following a maternal dose of 50 mg per day (Liedholm 1983). Cyanosis and bradycardia in a 5-day-old term infant associated with maternal intake of 50 mg atenolol twice daily in breastmilk has been reported. The infant recovered when breastfeeding was interrupted (Schimmel et al. 1989). Other authors have reported no adverse effects in 15 infants aged 3 days to 2 weeks exposed to 50–100 mg atenolol (Bhamra et al. 1983; White et al. 1984; Kulas et al. 1984). It is not licensed for use in children under the age of 12 years. Relative infant dose quoted as 6.6% (Hale 2017 online access).
Atenolol has low plasma protein binding and therefore passes more freely into breastmilk. Caution is particularly advised in neonates because of the renal excretion of this drug.
Labetolol; Michael’s study of 25 patients (1979) taking between 330 and 800 mg labetolol daily showed a m/p ratio less than 1, although one patient taking 1200 mg daily produced milk samples where the concentration in milk exceeded that in maternal plasma. Lunell et al.’s study (1985) produced similar results. However, no baby in these studies exhibited any adverse drug reactions. Mirpuri et al. (2008) reported that a 26-week premature baby exhibited bradycardia and premature beats when tube fed expressed breastmilk from its mother who was receiving 300 mg labetolol twice daily. Its condition returned to normal when formula milk was substituted. McGuinness identified that a mother’s intake of labetolol had triggered symptoms of Raynaud’s syndrome due to restriction of blood flow to the extremities. This should be borne in mind with any mum reporting panful breastfeeding when on beta blockers.
Metoprolol: Studies have shown that metoprolol also produces m/p ratios in excess of 1 (Sandström and Regårdh 1980; Liedholm et al. 1981). However, the absolute level of drug transferring to the baby is small and studies have failed to detect metoprolol at significant levels in infant plasma (Kuklas et al. 1984). Although the drug is well-absorbed, it undergoes extensive first-pass metabolism. No adverse events have been reported in babies exposed to metoprolol via breastmilk (Ho et al. 1999; Lindeberg et al. 1984
Bisoprolol: Only one study of the use of bisoprolol appears in the literature. Khurana studied a mother who was initiated on it 6 days after birth for a cardiac condition. She expressed samples of milk on day 11 and 18 after birth. Drug levels in milk were undetectable but the baby did not receive any breastmilk, so data is incomplete. See https://breastfeeding-and-medication.co.uk/fact-sheet/bisoprolol-and-breastfeeding
Propranolol: almost completely absorbed from the gastrointestinal tract but undergoes first-pass metabolism. It is highly lipid soluble and is approximately 90% plasma protein bound. It has at least one active metabolite but the impact of this is unclear.
In adults it may be used to lower blood pressure, to relieve symptoms of hyperthyroidism, to prevent migraines or to prevent panic attacks. See https://breastfeeding-and-medication.co.uk/thoughts/propranolol-and-breastfeeding
In a study of three women (Smith 1983) it was calculated that the maximum dose likely to be ingested by a breastfed infant would be less than 0.1% of the maternal dose.
Angiotensin II receptor antagonists
This group of drugs is given to patients who are unable to tolerate ACE inhibitors to treat hypertension and heart failure. As with ACE inhibitors, this group of drugs is contra-indicated in pregnancy. There are few data on transfer into breastmilk and the use of ACE inhibitors is recommended. This class of drug might be expected to produce low levels in breastmilk because of the high protein binding and low bioavailability but no data exist to support this assumption.
Candestartan : has limited oral bio availability of 14%, and a plasma protein binding > 99%. There is one study of 3 breastfeeding mothers, all stabilized on candesartan (8-32 mg daily ). They provided milk and plasma samples over 24 hours. Plasma samples were obtained from 2 of the babies The relative infant dose was estimated to be 0.09%. Candesartan was undetectable (less than 0.2 micrograms/L) in infant plasma samples (Coberger 2019, LactMed).
Irbesartan; oral bio availability 60-80% and plasma protein binding 90%. Because no information is available on the use of irbesartan during breastfeeding it is best avoided. If a sartan is considered essential candesartan might be preferable
Losartan; oral bio availability of 33%, and high plasma protein binding of 99.8%. Kearney (2018) suggests that the high protein-binding of losartan and low oral bioavailability makes excretion into breast milk and subsequent absorption by the baby unlikely. She suggests that if the mother has developed Postpartum cardiomyopathy, breastfeeding need not be discouraged. However, there are no relevant published data on excretion into breast milk.
Valsartan; has an oral bio availability 23%, and plasma protein binding of 95%. There are no relevant published data on excretion into breast milk. Candesartan may be seen as the best option if a sartan is considered essential.
Calcium channel blockers
Nifedipine: relaxes vascular smooth muscle and dilates coronary and peripheral arteries. It has activity in reducing blood pressure and in the treatment of Reynaud’s syndrome. Nifedipine is almost completely absorbed from the GI tract but undergoes extensive first-pass metabolism. Side effects for the mother include flushing and headache, which may limit its usefulness. It is present in breastmilk but in levels too small to be harmful and there have been no reports of adverse effects in babies. See https://breastfeeding-and-medication.co.uk/fact-sheet/february-is-raynaud-s-awareness-month-www-sruk-co-uk
Amlodipine: A study of 31 postpartum women (Naito 2015) with pregnancy-induced hypertension received amlodipine 5 mg daily by mouth, with the dosage increased as needed to maintain blood pressure of 140/90 mm Hg or less (mean dosage for the group was 6 mg daily. Maternal blood and breastmilk samples were obtained after at least 6 days of therapy. The median milk concentration was 11.5 µg/L, and no infant showed any adverse effects.
Felodipine: Small amounts of felodipine may get into breast milk, but it’s not known if this is harmful to the baby (BNF). Oral bio availability 20%, plasma protein binding >99%, no studies of passage into breastmilk have been located
Diltiazem: Diltiazem is used for its antiarrhythmic, anti-anginal and antihypertensive properties but rarely in women of childbearing age unless there are very specific indications from the medical history. It is rarely used simply to treat hypertension.
Alpha blockers
Avoid unless essential to mother’s health. This class of drugs are generally only used in addition to other drugs with poorly controlled blood pressure. They are not normally used as first line or monotherapy
Doxazosin: Jensen published a paper on one mother breastfeeding a 6-month-old. She received 4 mg daily for 2 days. The maximum milk concentrations were 2.9 and 4.2 µg/L. This drug should only be used in extreme circumstances and with close monitoring of the infant, for drowsiness, poor feeding, low blood pressure.
Terazosin: no studies in breastfeeding. Terazosin has rather powerful effects on the prostate and testes producing testicular atrophy in some animal studies (particularly new-born) and is therefore not preferred in pregnant or in lactating women (Hale)
NICE Guidance NG 133 (June 2019)
1.9 Antihypertensive treatment during the postnatal period, including during breastfeeding
1.9.1 Advise women with hypertension who wish to breastfeed that their treatment can be adapted to accommodate breastfeeding, and that the need to take antihypertensive medication does not prevent them from breastfeeding. [2019]
1.9.2 Explain to women with hypertension who wish to breastfeed that:
- antihypertensive medicines can pass into breast milk
- most antihypertensive medicines taken while breastfeeding only lead to very low levels in breast milk, so the amounts taken in by babies are very small and would be unlikely to have any clinical effect
- most medicines are not tested in pregnant or breastfeeding women, so disclaimers in the manufacturer’s information are not because of any specific safety concerns or evidence of harm.
- Make decisions on treatment together with the woman, based on her preferences. [2019]
1.9.3 As antihypertensive agents have the potential to transfer into breast milk:
- consider monitoring the blood pressure of babies, especially those born preterm, who have symptoms of low blood pressure for the first few weeks
- when discharged home, advise women to monitor their babies for drowsiness, lethargy, pallor, cold peripheries or poor feeding. [2019]
1.9.4 Offer enalapril [5]to treat hypertension in women during the postnatal period, with appropriate monitoring of maternal renal function and maternal serum potassium. [2019]
1.9.5 For women of black African or Caribbean family origin with hypertension during the postnatal period, consider antihypertensive treatment with: nifedipine [3] or amlodipine if the woman has previously used this to successfully control her blood pressure. [2019]
1.9.6 For women with hypertension in the postnatal period, if blood pressure is not controlled with a single medicine, consider a combination of nifedipine [3] (or amlodipine) and enalapril [5]. If this combination is not tolerated or is ineffective, consider either: adding atenolol or labetalol to the combination treatment or swapping 1 of the medicines already being used for atenolol or labetalol. [2019]
1.9.7 When treating women with antihypertensive medication during the postnatal period, use medicines that are taken once daily when possible. [2019]
1.9.8 Where possible, avoid using diuretics or angiotensin receptor blockers [5] to treat hypertension in women in the postnatal period who are breastfeeding or expressing milk. [2010, amended 2019]
1.9.9 Treat women with hypertension in the postnatal period who are not breastfeeding and who are not planning to breastfeed in line with the NICE guideline on hypertension in adults. [2019]
Inflammatory Bowel Disease and Breastfeeding
Many people know that I have had Crohns disease since I was 22 years old – that was when it was officially diagnosed but probably from 4 years before when I was 18 years old. It has had an immense effect on my life firstly medically – I have had 3 bowel resections and been on medications since the last one in 2002 which very nearly killed me. The only times when I was really fit in and well were when I was pregnant and breastfeeding which sparked my interest in becoming a breastfeeding counsellor 35 years ago. It meant I fed my second and third daughters for much longer (I became very ill soon after I weaned my first) and became passionate about supporting women to breastfeed. As a pharmacist that rolled into an interest and then passion about drugs in breastmilk.
When I regularly had contact with mums with IBD asking about their medication I decided to set up the Facebook group as a mutual support group. Mums who understood the urgency of toilet visits when out shopping, understood how debilitating it was to be in constant pain, that we could discuss anything in a private forum with others in the same situation. Coincidentally it has become a place where people ask each other about drugs and look to me to provide evidence of safety in breastfeeding – that wasn’t the original intent but an excellent spin off.
I havent set up any other specialist interest groups – this is out of my personal interest. Unsurprisingly the diagnosis and treatment of inflammatory bowel disease has taken up a lot of space in my book Breastfeeding and Medication and I am keen that professionals understand that breastfeeding protects our babies but is also something which we value above many things.
As of this morning we have 1.6K members from all over the world, climbing steeply recently January 2022).
Specialists seem to be very concerned about the safety of the drugs – which are strong admittedly and breastfeeding. But we also need to bear in mind that IBD is at least partly linked with being formula fed so we want to maintain breastfeeding and use specialist sources.
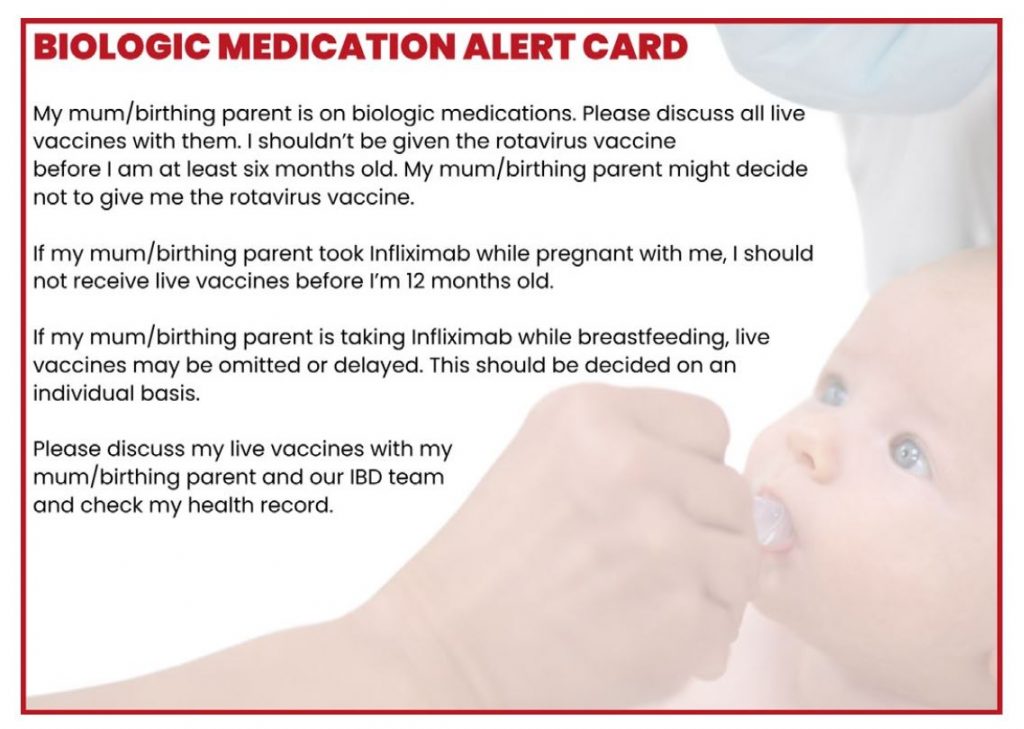
Live vaccines may be delayed or omitted – particularly the rotavirus vacc. However, this is as much to protect the mother who may contract the illness from the viral particles shed through the faeces, Exclusively breastfed babies are at low risk if contracting rotavirus in any case.
I am going to admit that I am passionate about the subject – this is the core of my life
See also Facebook live video
CONCLUSIONS: In a study of women receiving treatment for IBD and their infants, we detected low concentrations of infliximab, adalimumab, certolizumab, natalizumab, and ustekinumab in breast milk samples. We found breastfed infants of mothers on biologics, immunomodulators, or combination therapies to have similar risks of infection and rates of milestone achievement compared with non-breastfed infants or infants unexposed to these drugs. Maternal use of biologic therapy appears compatible with breastfeeding.
With the help of the Breastfeeding and IBD facebook page I wrote this article:
what would you like your healthcare tean to know about IBD and breastfeeding
Finally I have put together all the information on studies on anything to do with prescribing, procedures and vaccines for breastfeeding mums with IBD. If you have IBD take this with you to appointments. If you are a professional please make sure everyone in the team has a copy. I am happy to offer Teams Training to any group of professionals who support mums with IBD.
All you need to know about investigating and treating IBD in breastfeeding mothers factsheet